

Hemodynamic impact of coronary stenosis using computed tomography: comparison between noninvasive fractional flow reserve and 3D fusion of coronary angiography with stress myocardial perfusion
- PMID: 31073698
- PMCID: PMC7081838
- DOI: 10.1007/s10554-019-01618-5
Hemodynamic impact of coronary stenosis using computed tomography: comparison between noninvasive fractional flow reserve and 3D fusion of coronary angiography with stress myocardial perfusion
Abstract
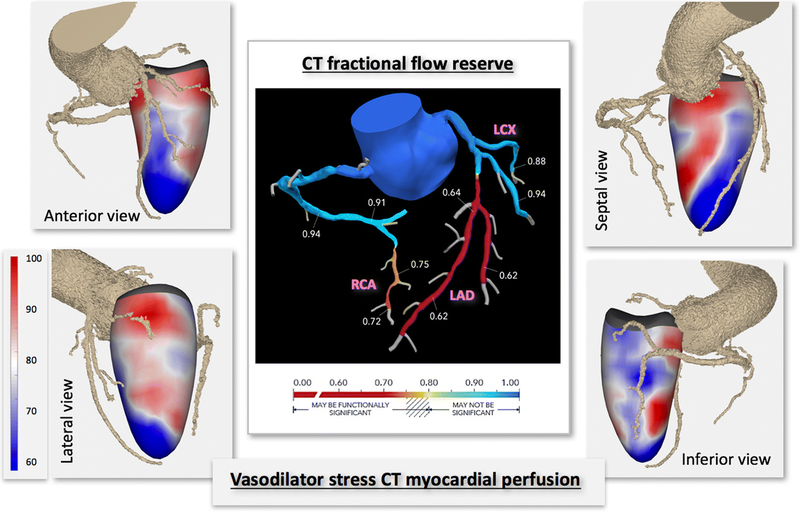
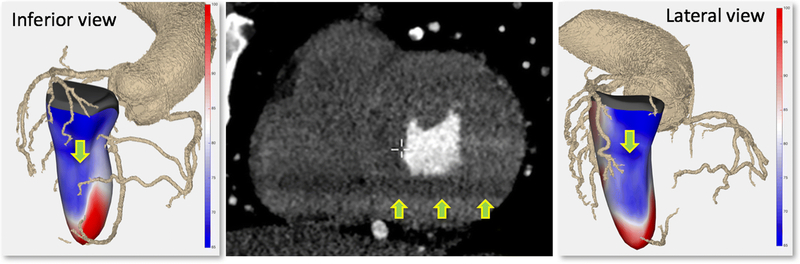
Vasodilator-stress CT perfusion imaging in addition to CT coronary angiography (CTCA) may provide a single-test alternative to nuclear stress testing, commonly used to assess hemodynamic significance of stenosis. Another alternative is fractional flow reserve (FFR) calculated from cardiac CT images. We studied the concordance between these two approaches and their relationship to outcomes. We prospectively studied 150 patients with chest pain, who underwent CTCA and regadenoson CT. CTCA images were interpreted for presence and severity of stenosis. Fused 3D displays of subendocardial X-ray attenuation with coronary arteries were created to detect stress perfusion defects (SPD) in each coronary territory. In patients with stenosis > 25%, CT-FFR was quantified. Significant stenosis was determined by: (1) combination of stenosis > 50% with an SPD, (2) CT-FFR ≤ 0.80. Patients were followed-up for 36 ± 25 months for death, myocardial infarction or revascularization. After excluding patients with normal arteries and technical/quality issues, in final analysis of 76 patients, CTCA depicted stenosis > 70% in 13/224 arteries, 50-70% in 24, and < 50% in 187. CT-FFR ≤ 0.80 was found in 41/224 arteries, and combination of SPD with > 50% stenosis in 31/224 arteries. Inter-technique agreement was 89%. Despite high incidence of abnormal CT-FFR (30/76 patients), only 7 patients experienced adverse outcomes; 6/7 also had SPDs. Only 1/9 patients with CT-FFR ≤ 0.80 but normal perfusion had an event. Fusion of CTCA and stress perfusion can help determine the hemodynamic impact of stenosis in one test, in good agreement with CT-FFR. Adding stress CT perfusion analysis may help risk-stratify patients with abnormal CT-FFR.
Keywords: Cardiovascular CT; Fusion imaging; Myocardial perfusion; Vasodilator stress.
Conflict of interest statement
Figures






References
-
- Garcia MJ, Lessick J, Hoffmann MH, Investigators CS (2006) Accuracy of 16-row multidetector computed tomography for the assessment of coronary artery stenosis. JAMA 296:403–411 - PubMed
-
- Miller JM, Rochitte CE, Dewey M et al. (2008) Diagnostic performance of coronary angiography by 64-row CT. N Engl J Med 359:2324–2336 - PubMed
-
- Schroeder S, Achenbach S, Bengel F et al. (2008) Cardiac computed tomography: indications, applications, limitations, and training requirements: report of a Writing Group deployed by the Working Group Nuclear Cardiology and Cardiac CT of the European Society of Cardiology and the European Council of Nuclear Cardiology. Eur Heart J 29:531–556 - PubMed
-
- Pijls NH, De Bruyne B, Peels K et al. (1996) Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. N Engl J Med 334:1703–1708 - PubMed
-
- Tonino PA, Fearon WF, De Bruyne B et al. (2010) Angiographic versus functional severity of coronary artery stenoses in the FAME study fractional flow reserve versus angiography in multivessel evaluation. J Am Coll Cardiol 55:2816–2821 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
