

Does the MDS-UPDRS provide the precision to assess progression in early Parkinson's disease? Learnings from the Parkinson's progression marker initiative cohort
- PMID: 31073716
- PMCID: PMC6647182
- DOI: 10.1007/s00415-019-09348-3
Does the MDS-UPDRS provide the precision to assess progression in early Parkinson's disease? Learnings from the Parkinson's progression marker initiative cohort
Abstract
Objectives: Developing disease modifying therapies for Parkinson's disease (PD) calls for outcome measurement strategies focused on characterizing early stage disease progression. We explored the psychometric evidence for using the Movement Disorder Society Unified Parkinson's Disease Rating Scale (MDS-UPDRS) part II (patient motor experience of daily living) and part III (clinician motor examination) in this context.
Methods: MDS-UPDRS-II and -III data were collected at screening, month 12, and month 24 from 384 early stage PD patients (diagnosis ≤ 2 years; Hoehn and Yahr stage 1/2) in the Parkinson's Progression Markers Initiative (PPMI) study. Psychometric analysis, based on Rasch measurement theory (RMT), was performed on both the original MDS UPDRS-II and -III scales and exploratory content-driven scale structures.
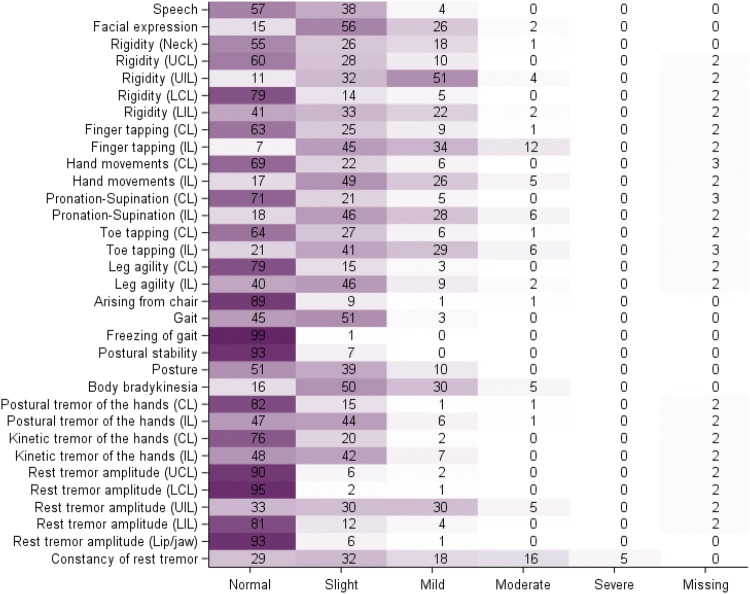
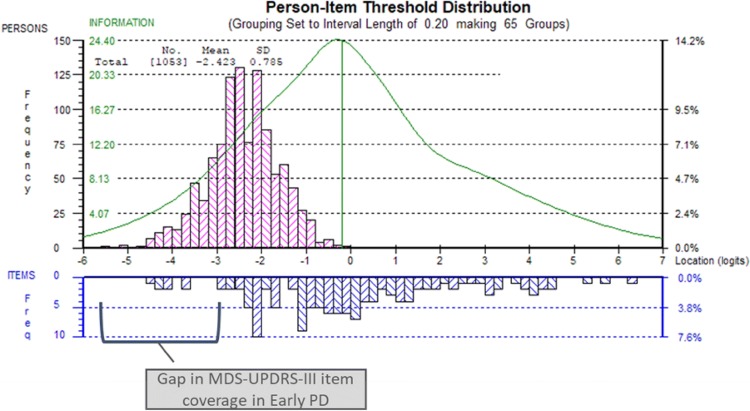
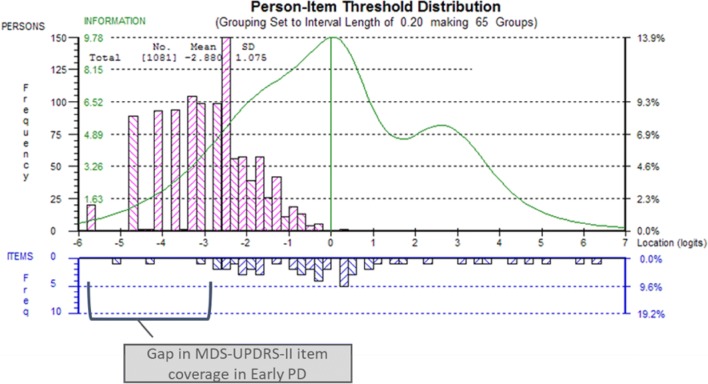
Results: RMT analyses showed neither scale was well targeted to early PD. A marked floor effect appeared for most items and a clear item gap was consistently observed in very mild severity of motor signs and levels of motor impact. The original MDS-UPDRS-II and -III scales also displayed disordered thresholds (9/13 and 20/33 items, respectively), indicating response scales not functioning as expected, and misfit (5/13 and 12/33 items, respectively), flagging areas for potential improvement.
Conclusions: The MDS-UPDRS-II and -III have psychometric limitations which limits the precision of measurement of motor symptoms and impact in early PD. This can lead to insensitivity in detecting differences and clinical change. Importantly, the diagnostic psychometric evidence provided by the RMT analysis provides a clear starting point for how to improve the quantification of clinically relevant concepts to characterize the course of early PD.
Keywords: Disease-modifying therapy; Early Parkinson’s disease; Movement Disorder Society Unified Parkinson’s Disease Rating Scale; Rasch measurement theory.
Conflict of interest statement
AR, JM and SC are employees of Modus Outcomes. BB, MB and TM are employees of UCB.
Figures

References
-
- Andrich D. An index of person separation in latent trait theory, the traditional KR. 20 index, and the Guttman scale response pattern. Educ Res Perspect. 1982;9:95–104.
-
- Andrich D. Rasch models for measurement. Newbury Park: Sage; 1988.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
