

Transaxillary robotic-assisted thyroid surgery: technique and results of a preliminary experience on the Da Vinci Xi platform
- PMID: 31074396
- PMCID: PMC7402570
- DOI: 10.1186/s12893-019-0473-0
Transaxillary robotic-assisted thyroid surgery: technique and results of a preliminary experience on the Da Vinci Xi platform
Abstract
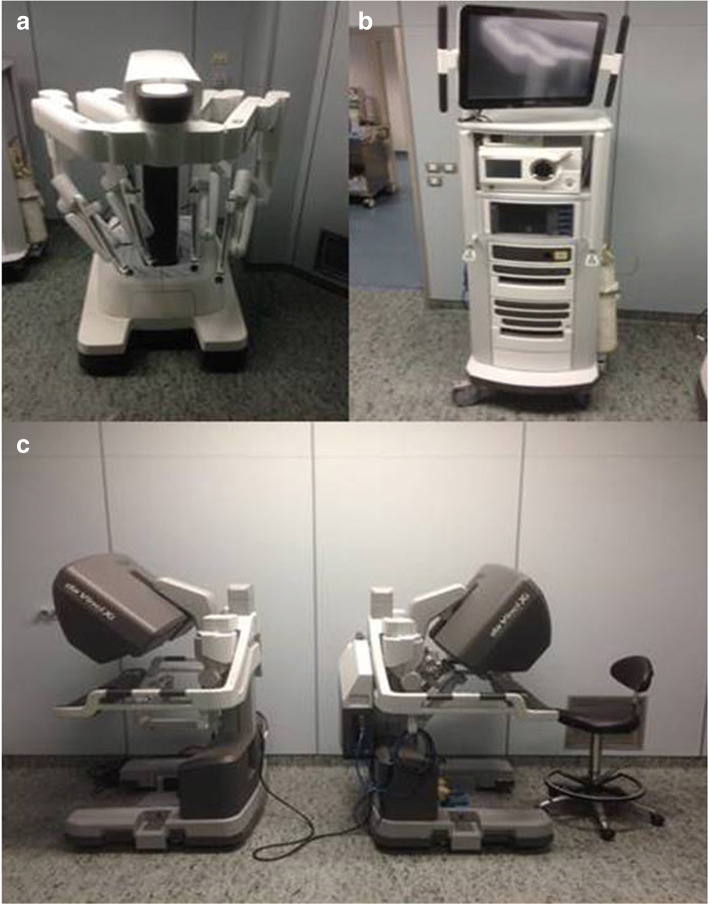
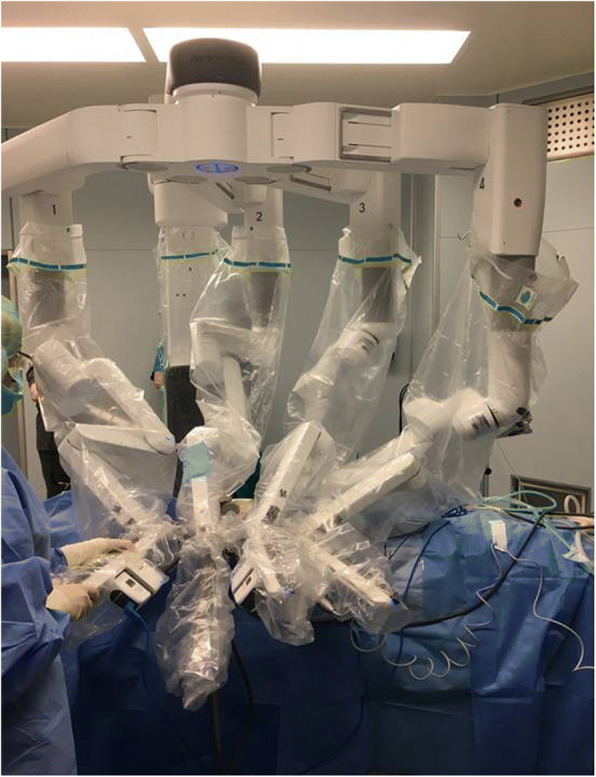
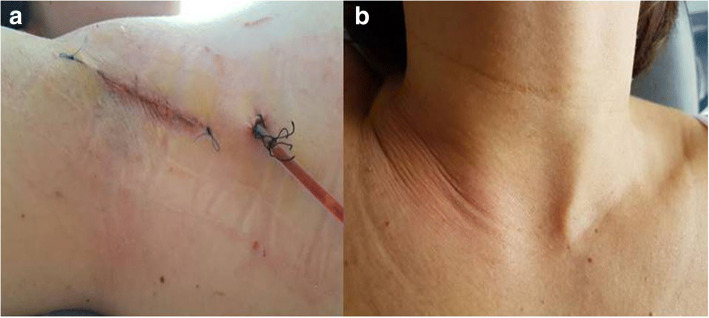
Background: Robotic thyroidectomy by transaxillary approach (RATS) is regarded as a feasible and safe alternative procedure in selected patients with benign disease or thyroid cancer of low risk, facilitating thyroidectomy with respect to conventional endoscopic approach and offering improved cosmetic results. The Da Vinci Xi surgical system (Intuitive Surgical, Sunnyvale, CA, USA) presents technical advantages over its previous generations, including overhead docking, more compact robotic arms, extended range of motion, and ability for camera to be docked in any arm. This construct supports dissection in smaller spaces with less arm interference and improved view. We present an initial experience of RATS on DVSS Xi in an academic Centre in Italy.
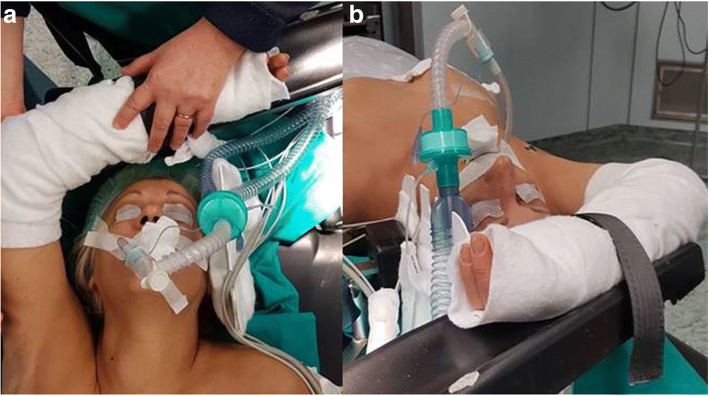
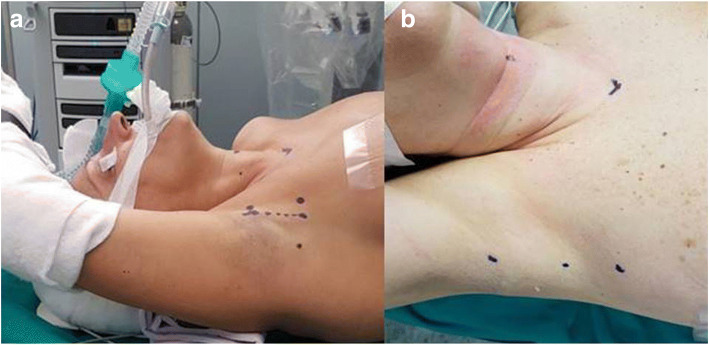
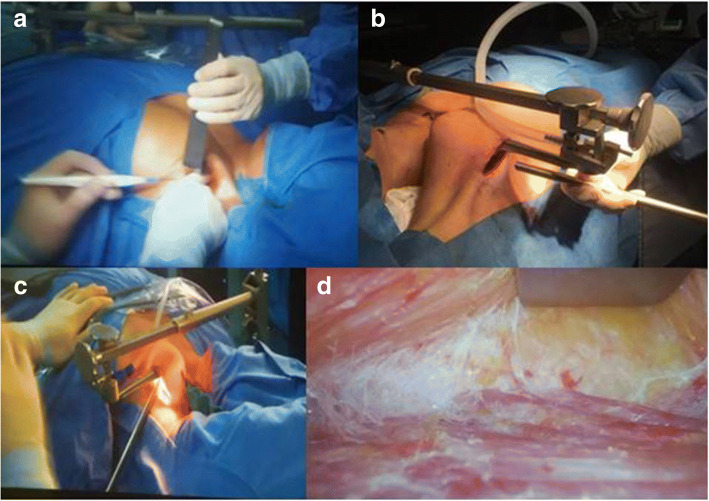
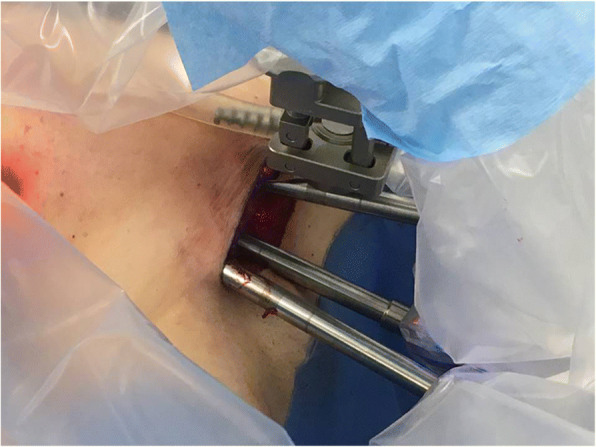
Methods: We conducted a prospective observational study, involving patients with thyroid disease and treated between April 2016 and January 2018. A modified thyroidectomy retractor (Modena retractor, CEATEC Medizintechnik, Germany) was used to lift a musculocutaneous flap and operate gasless. Instrument placement was recorded for each procedure. Each procedure description was broken down into three phases, creation of working space, machine docking with instrument positioning and endoscopic operating technique. Duration of cases was recorded. Patients selected were young women, BMI < 30, thyroid nodule < 5 cm, cytology TIR2 to TIR4 (TIR4:only nodules < 1 cm diameter).
Results: Twelve RATS were performed within the learning curve for the robotic technique, 10 lobectomies and 2 total thyroidectomies. No patients required reintervention. Mean duration of surgery was 198.9 min for lobectomy and 210 for thyroidectomy. The same surgical team performed all procedures. No patients presented surgery-related complications, mean stay was 3 days. Decrease in operating time was observed after 8 cases along with more precise preparation of working space. Four arms were used in the first 10 procedures then only three. No recurrent laryngeal nerve dysfunction, no seroma or haematoma were recorded. One patient had transient hypocalcaemia after total thyroidectomy.
Conclusions: Since the early phases of a preliminary experience RATS appeared a safe alternative to open thyroidectomy. Uptake of technique was quick on Xi platform with few technical tweaks over techniques described for Si machines. Careful patient selection is crucial.
Trial registration: Retrospectively registered on 20 july 2018 .
Trial registration number: researchregistry4272. The Research Registry: https://www.researchregistry.com/browse-the-registry#home/registrationdetails/5b517f08dbc2045aefd7f9b4/.
Keywords: Da Vinci Xi; Remote access surgery; Robotic-assisted; Thyroidectomy; Trans-axillary approach.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Ikeda Y, et al. Endoscopic resection of thyroid tumors by the axillary approach. J Cardiovasc Surg. 2000;41(5):791. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
