

The impact of the ultrasonic, bipolar and integrated energy devices in the adrenal gland surgery: literature review and our experience
- PMID: 31074403
- PMCID: PMC7402574
- DOI: 10.1186/s12893-018-0457-5
The impact of the ultrasonic, bipolar and integrated energy devices in the adrenal gland surgery: literature review and our experience
Abstract
Background: The gold standard approach for surgical treatment of benign and malignant adrenal lesion is considered the laparoscopic one, due to a lot of advantages compared to open approach. The rapid propagation of this surgical technique is due to the diffusion of haemostatic devices in laparoscopic adrenal surgery. The principal aim of this study is to analyze the outcome of LA using each energy modality, evaluating the eventual superiority of an instrument over the others.
Methods: A retrospective study, involving 75 consecutive patients submitted to LA by transperitoneal lateral approach from January 2013 to June 2017, was performed. Age less than 70 years old, adrenal adenomas less than 8 cm in diameter, incidentalomas < 6 cm, myelolipomas < 13 cm, adrenal metastases < 7 cm and ASA score ≤ III were the main surgical inclusion criteria. All involved patients were divided into three group, one for each energy device: group 1 - Harmonic Scalpel, group 2 - Ligasure vessel sealing system and group 3 - Thunderbeat. In each group only one device was applied for dissection and haemostasis during the whole operation. Each group consisted of 25 patients, well matched for histology, tumor size and site, gender and age. The following parameters were collected: age, gender, size of the tumor, side of the affected gland, pathology, operating time, intraoperative blood losses, hospitalization time, complication and conversion rate.
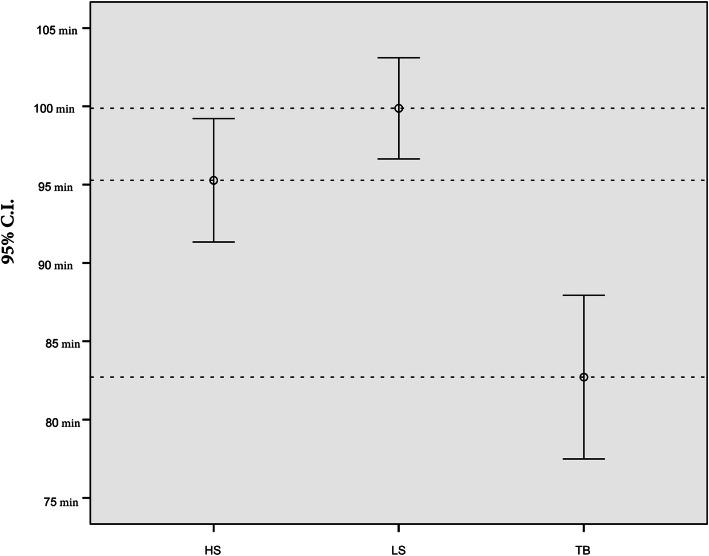
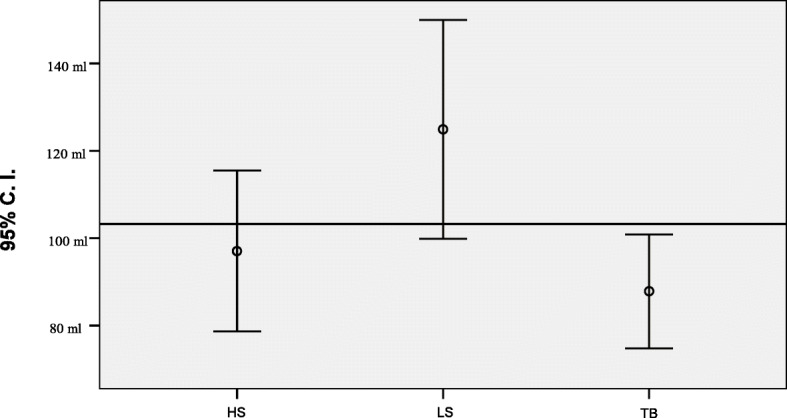
Results: There was no significant statistical difference between groups regarding the relationship between male/female, right site/left site, the mean age, hospitalization time and the tumor size (p > 0.05). Significant statistical difference are detectable in operation time and intraoperative blood losses. Thunderbeat, compared respectively with Ligasure and Harmonic Scalpel, is the fastest device (p < 0,001). The second faster device resulted Harmonic Scalpel, which meanly reduced the operation time compared to Ligasure (p = 0.048). intraoperative blood losses are reduced using Thunderbeat (p < 0,001) and HS (p = 0.006) compared to Ligasure, but between Thunderbeat and Harmonic Scalpel there isn't significant statistical difference (p = 0.178).
Conclusions: Analyzing the results, laparoscopic adrenalectomy carried out using Thunderbeat appeared to show a statistically significant decrease in operation time and intraoperative blood losses compared with laparoscopic adrenalectomy performed using Harmonic Scalpel and Ligasure, while hospitalization time was superimposable in all groups. According to our data, a responsible use of advanced energy devices can improve surgical outcomes guarantying a cost savings and patient's satisfaction.
Keywords: Harmonic Focus; Hemostatic devices; Laparoscopic adrenalectomy; Ligasure; Minimally invasive adrenalectomy; Thunderbeat.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- McLeod MK. Complications following adrenal surgery. J Natl Med Assoc. 1991;83(2):161–4. https://www.ncbi.nlm.nih.gov/pubmed/2005653. - PMC - PubMed
-
- Conzo G, Tartaglia E, Gambardella C, Esposito D, Sciascia V, Mauriello C, Nunziata A, Siciliano G, Izzo G, Cavallo F, Thomas G, Musella M, Santini L. Minimally invasive approach for adrenal lesions: systematic review of laparoscopic versus retroperitoneoscopic adrenalectomy and assessment of risk factors for complications. Int J Surg. 2016;28:118–123. doi: 10.1016/j.ijsu.2015.12.042. - DOI - PubMed
-
- Conzo G, Pasquali D, Gambardella C, Della Pietra C, Esposito D, Napolitano S, Tartaglia E, Mauriello C, Thomas G, Pezzolla A, De Bellis A, Santini L, Sinisi AA. Long-term outcomes of laparoscopic adrenalectomy for Cushing disease. Int J Surg. 2014;12:107–111. doi: 10.1016/j.ijsu.2014.05.036. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
