

Dietary Omega Polyunsaturated Fatty Acid Intake and Patient-Reported Outcomes in Systemic Lupus Erythematosus: The Michigan Lupus Epidemiology and Surveillance Program
- PMID: 31074595
- PMCID: PMC6842394
- DOI: 10.1002/acr.23925
Dietary Omega Polyunsaturated Fatty Acid Intake and Patient-Reported Outcomes in Systemic Lupus Erythematosus: The Michigan Lupus Epidemiology and Surveillance Program
Abstract
Objective: To examine associations between dietary intake of omega-3 (n-3; generally antiinflammatory) and omega-6 (n-6; generally proinflammatory) fatty acids and patient-reported outcomes in systemic lupus erythematosus (SLE).
Methods: This study was based on the population-based Michigan Lupus Epidemiology and Surveillance cohort. Estimates of n-3 and n-6 intake were derived from Diet History Questionnaire II items (past year with portion size version). Patient-reported outcomes included self-reported lupus activity (Systemic Lupus Activity Questionnaire [SLAQ]). Multivariable regression, adjusted for age, sex, race, and body mass index, was used to assess associations between absolute intake of n-3 and n-6, as well as the n-6:n-3 ratio, and patient-reported outcomes.
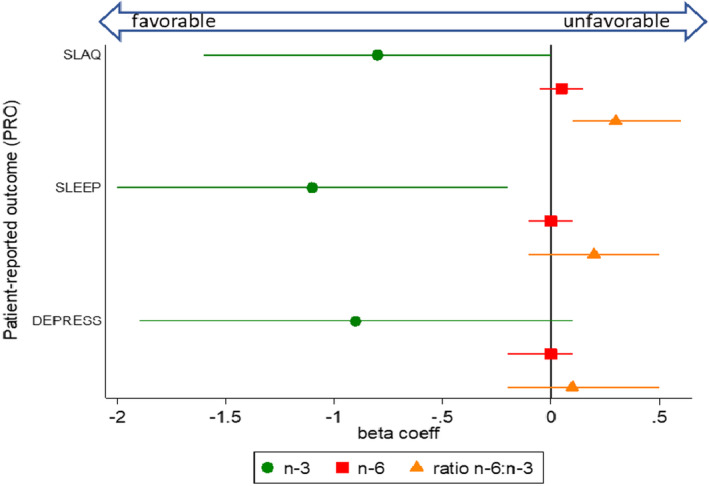
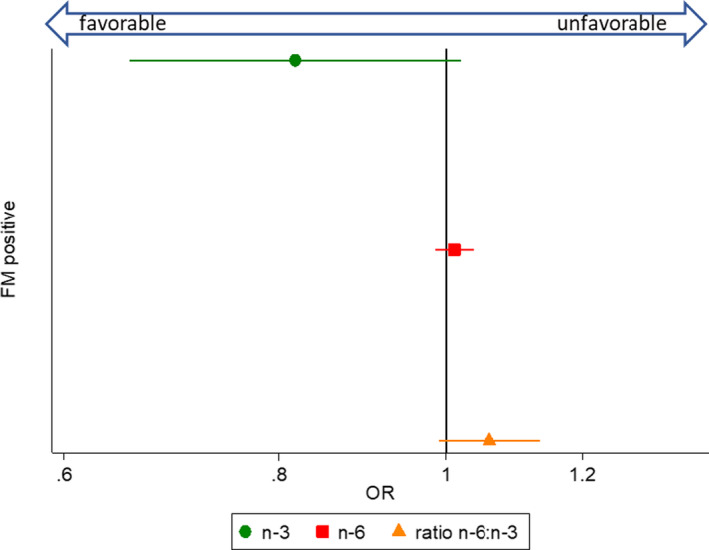
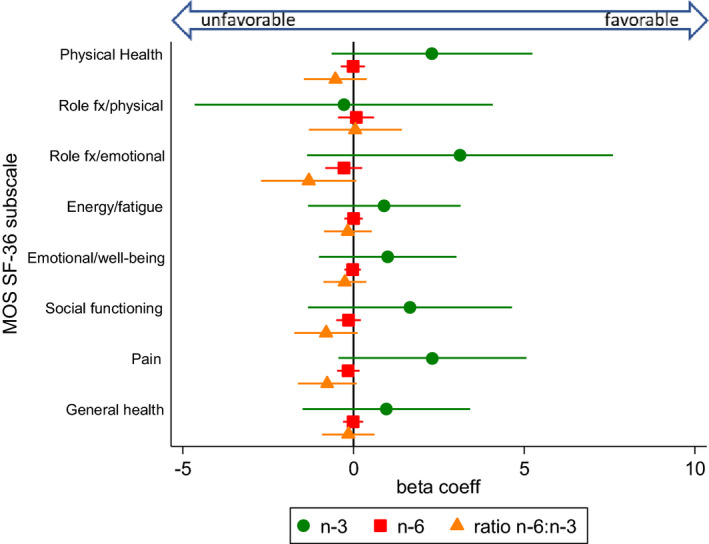
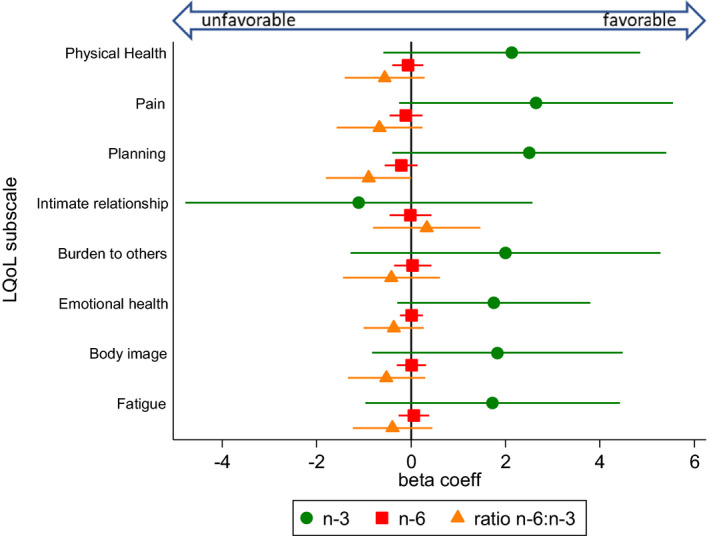
Results: Among 456 SLE cases, 425 (93.2%) were female, 207 (45.4%) were African American, and the mean ± SD age was 52.9 ± 12.3 years. Controlling for potential confounders, the average SLAQ score was significantly higher by 0.3 points (95% confidence interval [95% CI] 0.1, 0.6; P = 0.013) with each unit increase of the n-6:n-3 ratio. Both lupus activity and Patient-Reported Outcomes Measurement Information System (PROMIS) sleep disturbance scores were lower with each 1-gram/1,000 kcal increase of n-3 fatty acids (SLAQ regression coefficient β = -0.8 [95% CI -1.6, 0.0]; P = 0.055; PROMIS sleep β = -1.1 [95% CI -2.0, -0.2]; P = 0.017). Higher n-3 intakes were nonsignificantly associated with lower levels of depressive symptoms and comorbid fibromyalgia, and with higher quality of life, whereas results for the n6:n3 ratio trended in the opposite direction.
Conclusion: This population-based study suggests that higher dietary intake of n-3 fatty acids and lower n-6:n-3 ratios are favorably associated with patient-reported outcomes in SLE, particularly self-reported lupus activity and sleep quality.
© 2019, The Authors. Arthritis Care & Research published by Wiley Periodicals, Inc. on behalf of American College of Rheumatology.
Figures
References
-
- Van der Heijde D, Daikh DI, Betteridge N, Burmester GR, Hassett AL, Matteson EL, et al. Common language description of the term rheumatic and musculoskeletal diseases (RMDs) for use in communication with the lay public, healthcare providers, and other stakeholders endorsed by the European League Against Rheumatism (EULAR) and the American College of Rheumatology (ACR). Arthritis Rheumatol 2018;70:826–31. - PubMed
-
- Bertsias GK, Salmon JE, Boumpas DT. Therapeutic opportunities in systemic lupus erythematosus: state of the art and prospects for the new decade. Ann Rheum Dis 2010;69:1603–11. - PubMed
-
- Zonana‐Nacach A, Roseman JM, McGwin G, Friedman AW, Baethge BA, Reveille JD, et al. Systemic lupus erythematosus in three ethnic groups. VI: Factors associated with fatigue within 5 years of criteria diagnosis. LUMINA Study Group. LUpus in MInority populations: NAture vs Nurture. Lupus 2000;9:101–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
