

Effect of Electronic Screening With Personalized Feedback on Adolescent Health Risk Behaviors in a Primary Care Setting: A Randomized Clinical Trial
- PMID: 31074815
- PMCID: PMC6512281
- DOI: 10.1001/jamanetworkopen.2019.3581
Effect of Electronic Screening With Personalized Feedback on Adolescent Health Risk Behaviors in a Primary Care Setting: A Randomized Clinical Trial
Abstract
Importance: Health risk behaviors are a leading cause of morbidity during adolescence. Screening and counseling for health risk behaviors are recommended but infrequently performed.
Objective: To test the effect of an electronic screening and feedback tool on clinician counseling and adolescent-reported health risk behaviors.
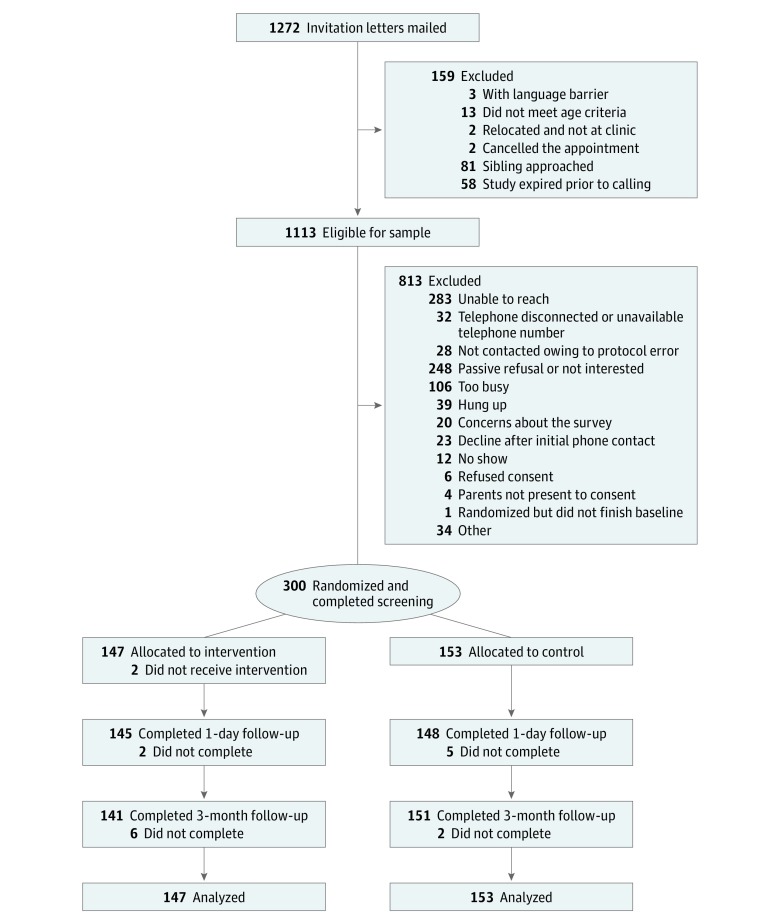
Design, setting, and participants: A randomized clinical trial compared electronic screening and feedback on an intention-to-treat basis with usual care among 300 youths 13 to 18 years of age at 5 pediatric clinics in the Pacific Northwest. Outcomes were assessed via electronic survey at 1 day and 3 months after the initial visit. Study data collection occurred from March 13, 2015, to November 29, 2016, and statistical analysis was conducted between February 6, 2017, and June 20, 2018.
Interventions: Youths in the intervention group (n = 147) received electronic screening and personalized feedback with clinician clinical decision support. Youths in the control group (n = 153) received standard screening and counseling as provided by their clinic.
Main outcomes and measures: Youths' report of receipt of counseling during the visit and risk behaviors at 3 months.
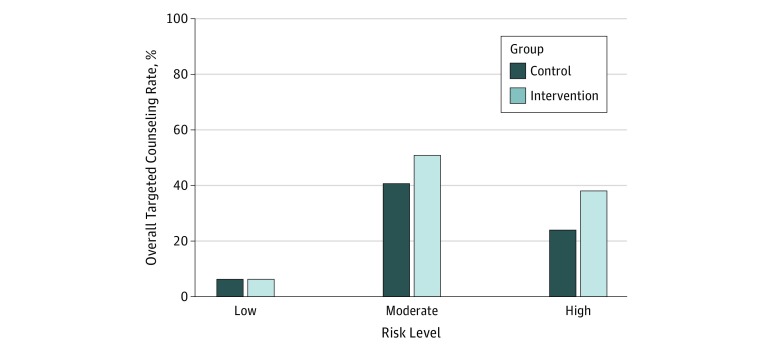
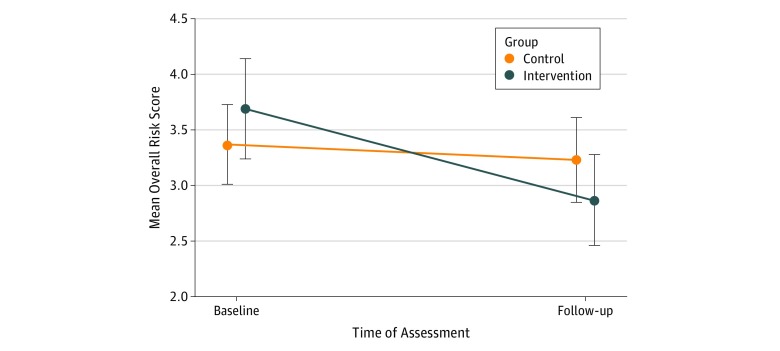
Results: In the final study sample of 300 youths (intervention group, 75 girls and 72 boys; mean [SD] age, 14.5 [1.4 years]; and control group, 80 girls and 73 boys; mean [SD] age, 14.5 [1.4] years), 234 (78.0%) were aged 13 to 15 years. After adjusting for age, sex, and random effect of clinic, youths in the intervention group were more likely to receive counseling for each of their reported risk behaviors than were youths in the control group (adjusted rate ratio, 1.32; 95% CI, 1.07-1.63). Youths in the intervention group had a significantly greater reduction (β = -0.48; 95% CI, -0.89 to -0.02; P = .02) in their risk behavior scores at 3 months when compared with youths in the control group.
Conclusions and relevance: Electronic screening of health risk behavior with clinical decision support and motivational feedback to teens can improve care delivery and outcomes.
Trial registration: ClinicalTrials.gov identifier: NCT02360410.
Conflict of interest statement
Figures
References
-
- Green M, Palfrey J, eds. Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents. 2nd ed Arlington, VA: National Center for Education in Maternal and Child Health; 2000.
-
- Elster A, Kuznets N, eds. Guidelines for Adolescent Preventive Services (GAPS). Baltimore, MD: Wiliams & Wilkins; 1994.
