

Assessment of the Feasibility and Cost of Hepatitis C Elimination in Pakistan
- PMID: 31074817
- PMCID: PMC6512462
- DOI: 10.1001/jamanetworkopen.2019.3613
Assessment of the Feasibility and Cost of Hepatitis C Elimination in Pakistan
Abstract
Importance: Chronic hepatitis C virus (HCV) infection is a global health problem. The World Health Assembly recently pledged to eliminate HCV by 2030. However, in Pakistan, a country with one of the highest prevalence rates, the feasibility and cost of HCV elimination are not known.
Objectives: To investigate whether and under what conditions HCV elimination is feasible in Pakistan and to estimate the cost of such elimination.
Design, setting, and participants: This decision analytical model study used a microsimulation model of the HCV epidemic in Pakistan from 2015 to 2030. Using Pakistan-specific variables, the model simulated the landscape of HCV in Pakistan and evaluated the minimum required screening and treatment rates needed to eliminate HCV in Pakistan. The study used simulated individuals chronically infected with HCV from 2015 to 2030. The analysis was performed in 2018.
Interventions: The status quo and 7 scenarios that can lead to HCV elimination in Pakistan by 2030, which were defined by different combinations of tests for screening, detection of viremia before treatment, and confirmation of treatment response.
Main outcomes and measures: Temporal trends in HCV infection prevalence, mortality, and disability-adjusted life-years and total cost of HCV infection care under the status quo and scenarios that can eliminate HCV by 2030.
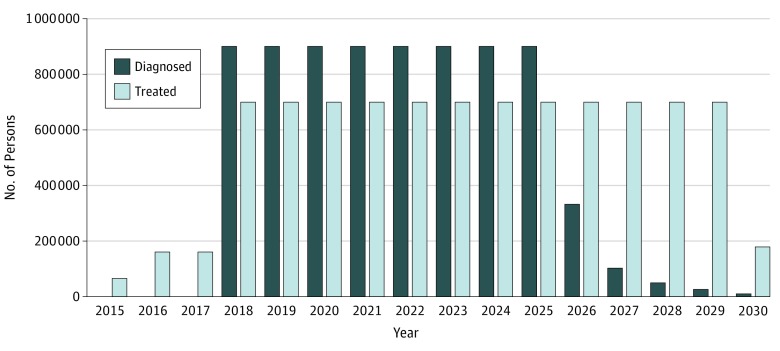
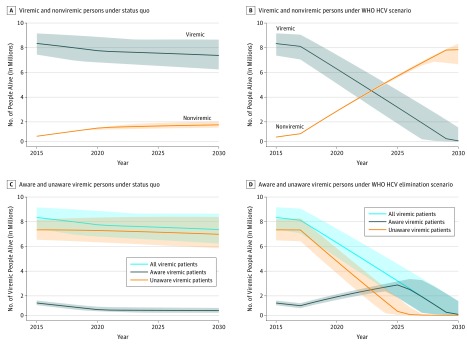
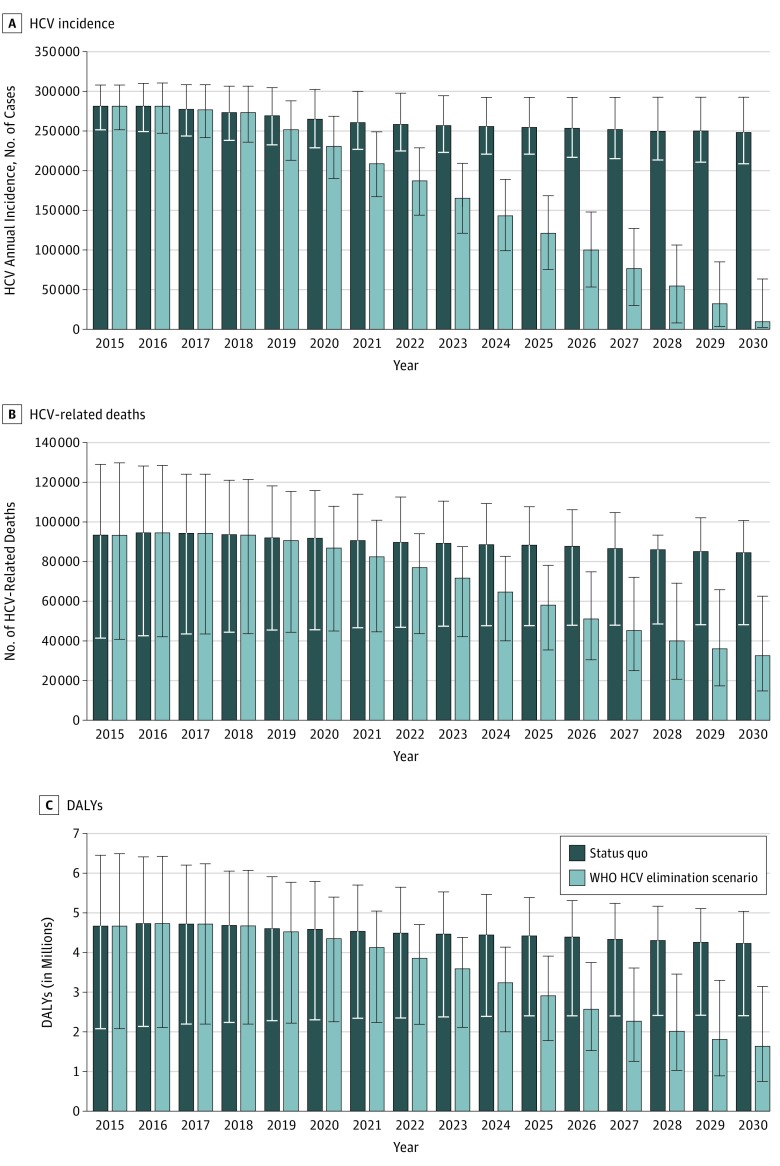
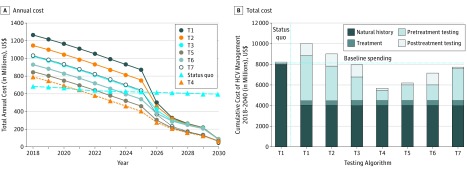
Results: Under the status quo, from 2015 to 2030, 1.44 million people are projected to die of HCV infection; 48% of deaths would be among people younger than 50 years. To achieve HCV elimination in Pakistan, HCV testing would need to be scaled up to at least 25 million people to diagnose 900 000 persons and treatment to 700 000 people per year. Compared with the status quo, the elimination scenario would avert 323 000 liver-related deaths and 13.0 million HCV-associated disability-adjusted life-years from 2015 to 2030. The elimination scenario was associated with cost savings of $2.6 billion from 2018 to 2030 with use of a point-of-care test for population-wide antibody screening and detection of viremia and treatment response.
Conclusions and relevance: Substantial scale-up of HCV testing and treatment may be essential to eliminate HCV infection in Pakistan, and such a strategy may be associated with cost savings in the near future. Although HCV elimination in Pakistan may be ambitious, strategic planning and strong support from the government may aid in its elimination.
Conflict of interest statement
Figures
References
-
- Degenhardt L, Peacock A, Colledge S, et al. Global prevalence of injecting drug use and sociodemographic characteristics and prevalence of HIV, HBV, and HCV in people who inject drugs: a multistage systematic review. Lancet Glob Health. 2017;5(12):e1192-e1207. doi: 10.1016/S2214-109X(17)30375-3 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
