

Association of Adult Congenital Heart Disease With Pregnancy, Maternal, and Neonatal Outcomes
- PMID: 31074818
- PMCID: PMC6512464
- DOI: 10.1001/jamanetworkopen.2019.3667
Association of Adult Congenital Heart Disease With Pregnancy, Maternal, and Neonatal Outcomes
Abstract
Importance: With the help of medical advances, more women with adult congenital heart disease (ACHD) are becoming pregnant. Adverse maternal, obstetric, and neonatal events occur more frequently in women with ACHD than in the general obstetric population. Adult congenital heart disease is heterogeneous, yet few studies have assessed whether maternal and neonatal outcomes differ across ACHD subtypes.
Objective: To assess the association of ACHD and its subtypes with pregnancy, maternal, and neonatal outcomes.
Design, setting, and participants: This cross-sectional study used data from the Discharge Abstract Database, which contains information on all hospitalizations in Canada (except Quebec) from fiscal years 2001-2002 through 2014-2015. Discharge Abstract Database information was linked with maternal and infant hospital records across Canada. All women who gave birth in hospitals during the study period were included in the study. Data were analyzed from December 18, 2017, to March 22, 2019.
Exposures: Women with ACHD were identified using diagnostic and procedural codes. Subtypes of ACHD were classified using the Anatomic and Clinical Classification of Congenital Heart Defects scheme.
Main outcomes and measures: Primary outcomes were defined a priori and included severe maternal morbidity (measured using the Maternal Morbidity Outcomes Indicator), neonatal morbidity and mortality (measured using the Neonatal Adverse Outcomes Indicator), ischemic placental disease, preterm birth, congenital anomalies, and small-for-gestational-age births. Absolute and relative rates of each outcome were calculated overall and by ACHD subtype. Logistic regression using generalized estimating equations assessed crude and adjusted odds ratios (aORs) for each outcome in women with ACHD compared with women without ACHD after adjustment for comorbidities, mode of delivery, and study year.
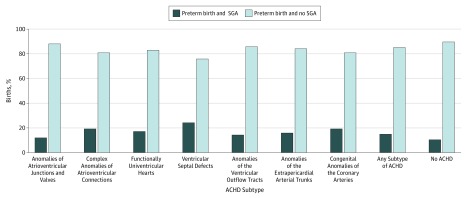
Results: The 2114 women with ACHD included in the analysis (mean [SD] age, 29.4 [5.7] years) had significantly higher odds of maternal morbidity (aOR, 2.7; 95% CI, 2.2-3.4) and neonatal morbidity and mortality (aOR, 1.8; 95% CI, 1.6-2.1) compared with women without ACHD (n = 2 682 451). Substantial variation was observed between women with different subtypes of ACHD. For example, the aORs of preterm birth (<37 weeks) varied from 0.4 (95% CI, 0.4-0.5) for women with anomalies of atrioventricular junctions and valves to 4.7 (95% CI, 2.9-7.5) for women with complex anomalies of atrioventricular connections.
Conclusions and relevance: These results suggest that women with different subtypes of ACHD are not uniformly at risk for adverse maternal and neonatal outcomes. Although some women with ACHD can potentially expect healthy pregnancies, it appears that clinical care should be modified to address the heightened risks of certain ACHD subtypes.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
