

Expenditures and Health Care Utilization Among Adults With Newly Diagnosed Low Back and Lower Extremity Pain
- PMID: 31074820
- PMCID: PMC6512284
- DOI: 10.1001/jamanetworkopen.2019.3676
Expenditures and Health Care Utilization Among Adults With Newly Diagnosed Low Back and Lower Extremity Pain
Abstract
Importance: Low back pain (LBP) with or without lower extremity pain (LEP) is one of the most common reasons for seeking medical care. Previous studies investigating costs in this population targeted patients receiving surgery. Little is known about health care utilization among patients who do not undergo surgery.
Objectives: To assess use of health care resources for LBP and LEP management and analyze associated costs.
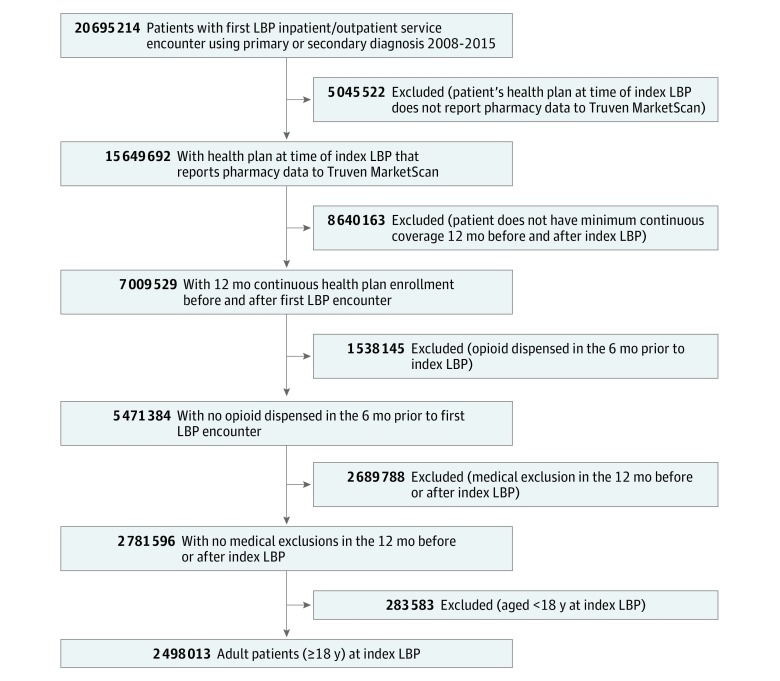
Design, setting, and participants: This cohort study used a retrospective analysis of a commercial database containing inpatient and outpatient data for more than 75 million individuals. Participants were US adults who were newly diagnosed with LBP or LEP between 2008 and 2015, did not have a red-flag diagnosis, and were opiate naive prior to diagnosis. Dates of analysis were October 6, 2018, to March 7, 2019.
Exposures: Newly diagnosed LBP or LEP.
Main outcomes and measures: The primary outcome was total cost of care within the first 6 and 12 months following diagnosis, stratified by whether patients received spinal surgery. An assessment was performed to determine whether patients who did not undergo surgery received care in accordance with proposed guidelines for conservative LBP and LEP management. Costs resulting from use of different health care services were estimated.
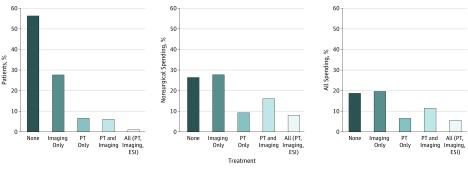
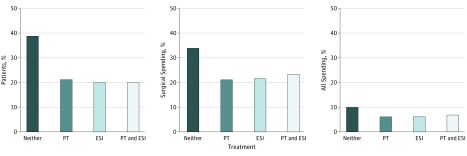
Results: A total of 2 498 013 adult patients with a new LBP or LEP diagnosis (median [interquartile range] age, 47 [36-58] years; 1 373 076 [55.0%] female) were identified. More than half (55.7%) received no intervention. Only 1.2% of patients received surgery, but they accounted for 29.3% of total 12-month costs ($784 million). Total costs of care among the 98.8% of patients who did not receive surgery were $1.8 billion. Patients who did not undergo surgery frequently received care that was inconsistent with clinical guidelines for LBP and LEP: 32.3% of these patients received imaging within 30 days of diagnosis and 35.3% received imaging without a trial of physical therapy.
Conclusions and relevance: The findings suggest that surgery is rare among patients with newly diagnosed LBP and LEP but remains a significant driver of spending. Early imaging in patients who do not undergo surgery was also a major driver of increased health care expenditures. Avoidable costs among patients with typically self-limited conditions result in considerable economic burden to the US health care system.
Conflict of interest statement
Figures
References
-
- Deyo RA, Mirza SK, Martin BI. Back pain prevalence and visit rates: estimates from U.S. national surveys, 2002. Spine (Phila Pa 1976). 2006;31(23):2724-2727. doi:10.1097/01.brs.0000244618.06877.cd - DOI - PubMed
-
- Dunn KM, Croft PR. Epidemiology and natural history of low back pain. Eura Medicophys. 2004;40(1):9-13. - PubMed
-
- Qaseem A, Wilt TJ, McLean RM, Forciea MA; Clinical Guidelines Committee of the American College of Physicians . Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017;166(7):514-530. doi:10.7326/M16-2367 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
