

Accumulated thermal dose in MRI-guided focused ultrasound for essential tremor: repeated sonications with low focal temperatures
- PMID: 31075781
- PMCID: PMC7139920
- DOI: 10.3171/2019.2.JNS182995
Accumulated thermal dose in MRI-guided focused ultrasound for essential tremor: repeated sonications with low focal temperatures
Abstract
Objective: The object of this study was to correlate lesion size with accumulated thermal dose (ATD) in transcranial MRI-guided focused ultrasound (MRgFUS) treatments of essential tremor with focal temperatures limited to 50°C-54°C.
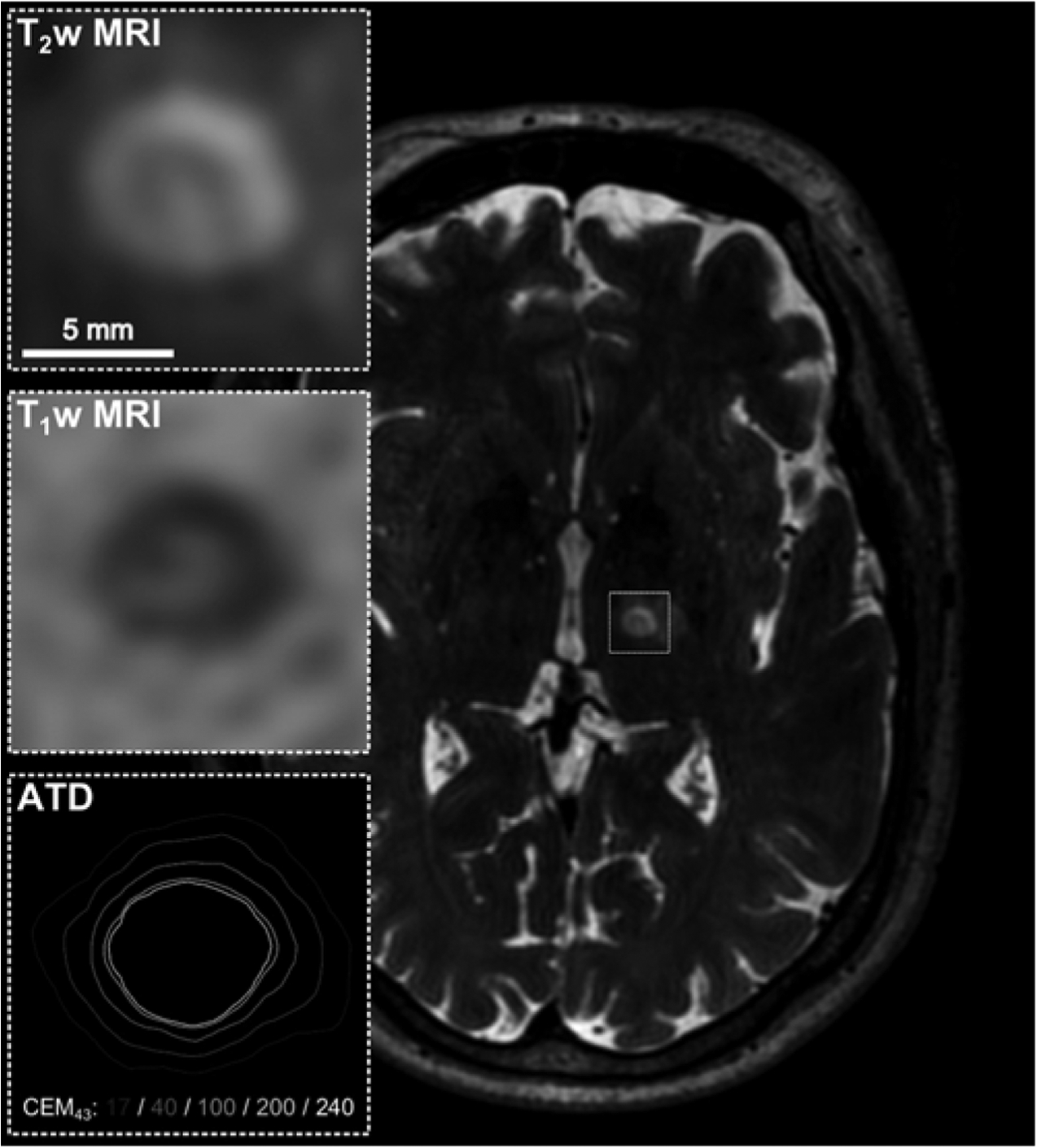
Methods: Seventy-five patients with medically refractory essential tremor underwent MRgFUS thalamotomy at the authors' institution. Intraoperative MR thermometry was performed to measure the induced temperature and thermal dose distributions (proton resonance frequency shift coefficient = -0.00909 ppm/°C). In 19 patients, it was not possible to raise the focal temperature above 54°C because of unfavorable skull characteristics and/or the pain associated with cranial heating. In this patient subset, sonications with focal temperatures between 50°C and 54°C were repeated (5.1 ± 1.5, mean ± standard deviation) to accumulate a sufficient thermal dose for lesion formation. The ATD profile sizes (17, 40, 100, 200, and 240 cumulative equivalent minutes at 43°C [CEM43]) calculated by combining axial MR thermometry data from individual sonications were correlated with the corresponding lesion sizes measured on axial T1-weighted (T1w) and T2-weighted (T2w) MR images acquired 1 day posttreatment. Manual corrections were applied to the MR thermometry data prior to thermal dose accumulation to compensate for off-resonance-induced spatial-shifting artifacts.
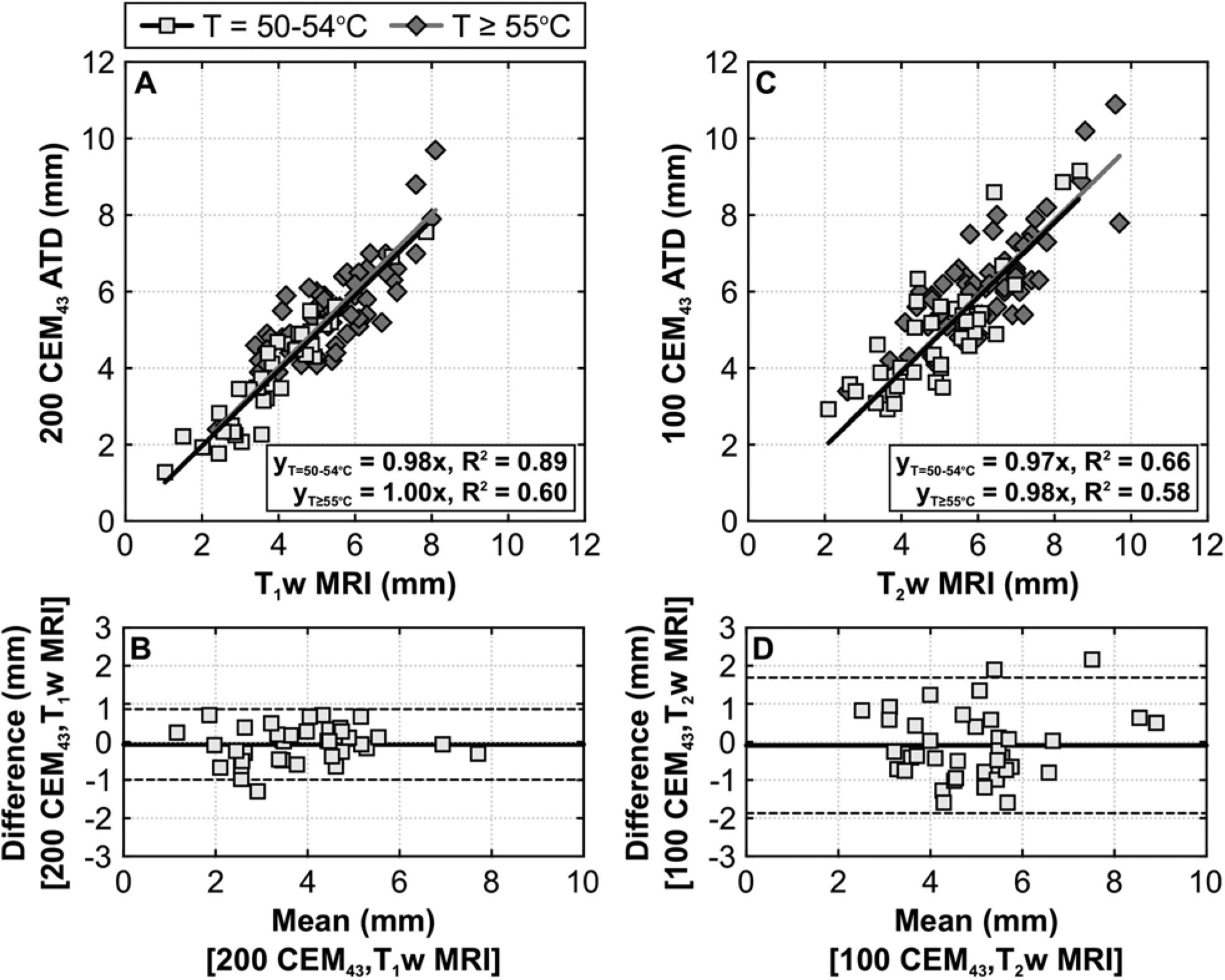
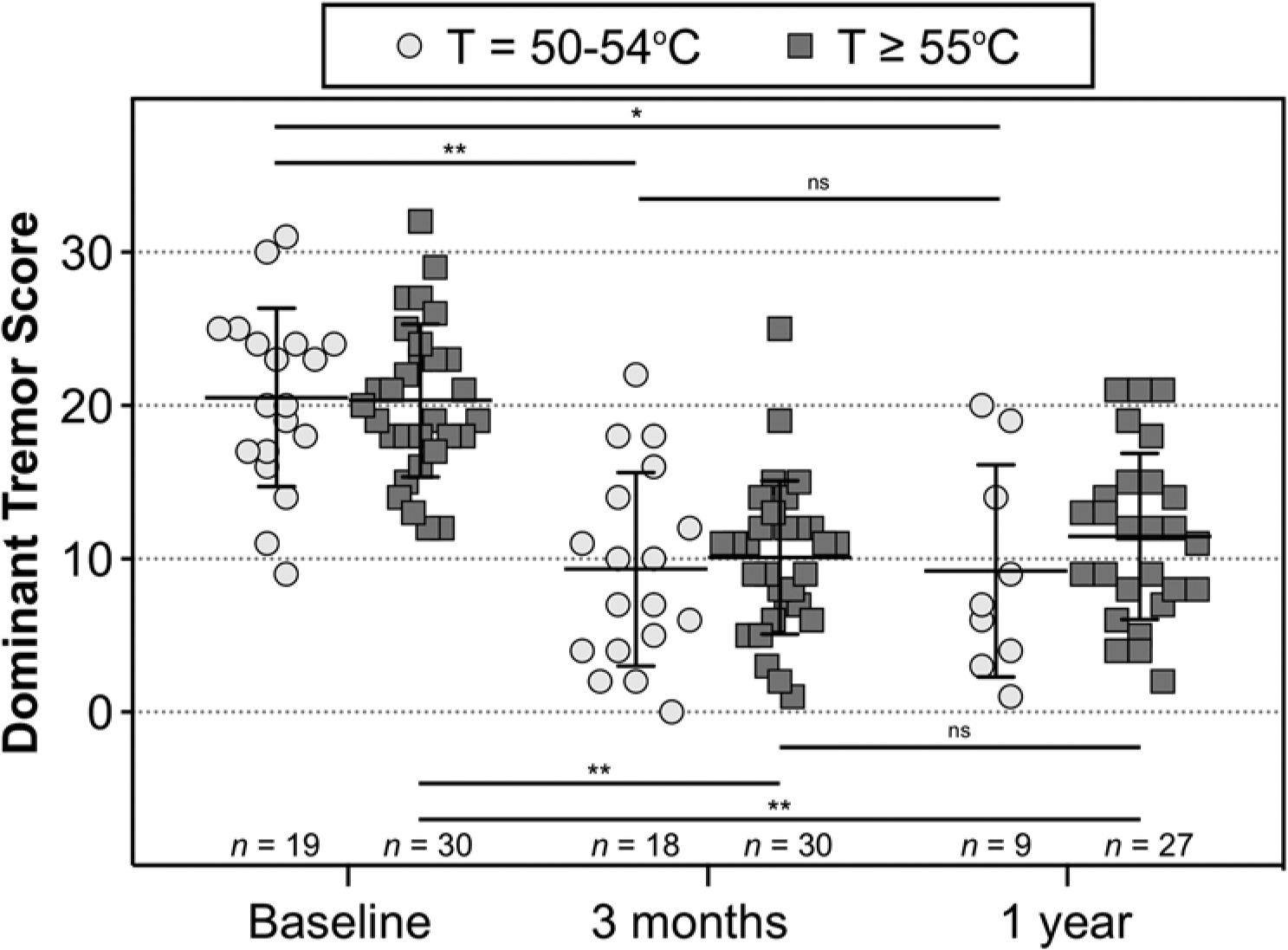
Results: Mean lesion sizes measured on T2w MRI (5.0 ± 1.4 mm) were, on average, 28% larger than those measured on T1w MRI (3.9 ± 1.4 mm). The ATD thresholds found to provide the best correlation with lesion sizes measured on T2w and T1w MRI were 100 CEM43 (regression slope = 0.97, R2 = 0.66) and 200 CEM43 (regression slope = 0.98, R2 = 0.89), respectively, consistent with data from a previous study of MRgFUS thalamotomy via repeated sonications at higher focal temperatures (≥ 55°C). Two-way linear mixed-effects analysis revealed that dominant tremor subscores on the Fahn-Tolosa-Marin Clinical Rating Scale for Tremor (CRST) were statistically different from baseline at 3 months and 1 year posttreatment in both low-temperature (50°C-54°C) and high-temperature (≥ 55°C) patient cohorts. No significant fixed effect on the dominant tremor scores was found for the temperature cohort factor.
Conclusions: In transcranial MRgFUS thalamotomy for essential tremor, repeated sonications with focal temperatures between 50°C and 54°C can accumulate a sufficient thermal dose to generate lesions for clinically relevant tremor suppression up to 1 year posttreatment, and the ATD can be used to predict the size of the resulting ablation zones measured on MRI. These data will serve to guide future clinical MRgFUS brain procedures, particularly those in which focal temperatures are limited to below 55°C.
Keywords: MR thermometry; focused ultrasound; functional neurosurgery; thalamotomy; thermal ablation; thermal dose.
Figures

References
-
- Bland JM, Altman DG: Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1:307–310, 1986 - PubMed
-
- Bond AE, Elias WJ: Predicting lesion size during focused ultrasound thalamotomy: a review of 63 lesions over 3 clinical trials. Neurosurg Focus 44(2):E5, 2018 - PubMed
-
- Boutet A, Ranjan M, Zhong J, Germann J, Xu D, Schwartz ML, et al. : Focused ultrasound thalamotomy location determines clinical benefits in patients with essential tremor. Brain 141:3405–3414, 2018 - PubMed
-
- Chang JW, Park CK, Lipsman N, Schwartz ML, Ghanouni P, Henderson JM, et al. : A prospective trial of magnetic resonance-guided focused ultrasound thalamotomy for essential tremor: results at the 2-year follow-up. Ann Neurol 83:107–114, 2018 - PubMed
-
- Chang WS, Jung HH, Kweon EJ, Zadicario E, Rachmilevitch I, Chang JW: Unilateral magnetic resonance guided focused ultrasound thalamotomy for essential tremor: practices and clinicoradiological outcomes. J Neurol Neurosurg Psychiatry 86:257–264, 2015 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
