

Review
doi: 10.1067/j.cpradiol.2019.04.003.
Epub 2019 Apr 8.
Tracheobronchial Tumors: Radiologic-Pathologic Correlation of Tumors and Mimics
Affiliations
- PMID: 31076268
- PMCID: PMC7115773
- DOI: 10.1067/j.cpradiol.2019.04.003
Item in Clipboard
Review
Tracheobronchial Tumors: Radiologic-Pathologic Correlation of Tumors and Mimics
Curr Probl Diagn Radiol.
2020 Jul-Aug.
Abstract
Tracheobronchial masses encompass a broad spectrum of entities, ranging from benign and malignant neoplasms to infectious and inflammatory processes. This article reviews the cross-sectional findings of tracheal tumors and tumor-like entities, correlates imaging findings with histologic pathology, and discusses pearls and pitfalls in accurately diagnosing and classifying tracheal tumors and mimics.
Copyright © 2019 Elsevier Inc. All rights reserved.
Figures

Normal larynx, trachea, and proximal bronchi opened from the posterior aspect.
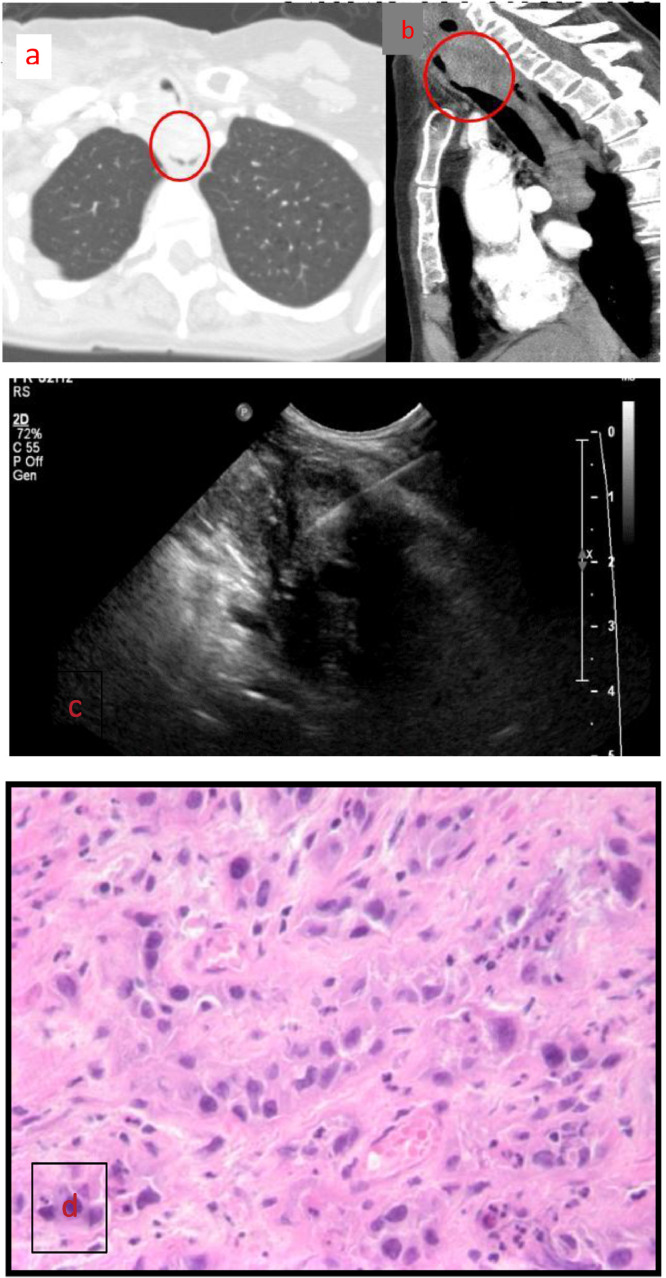
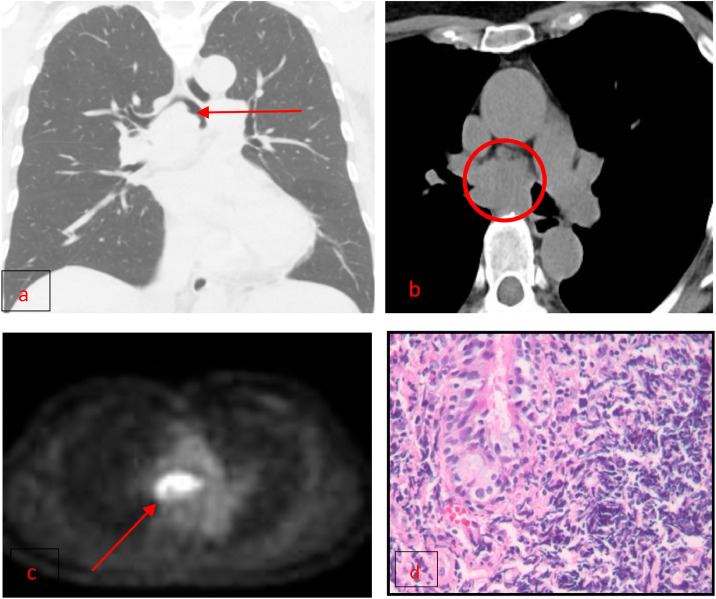
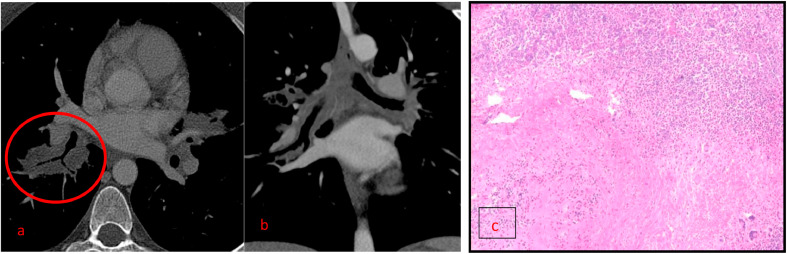
(a, b) Axial and sagittal CT images demonstrating squamous cell carcinoma centered in the superior trachea with posterior extension into the esophagus. (c) Ultrasound-guided biopsy of an enlarged right supraclavicular lymph node was performed. (d) Infiltration by large atypical neoplastic cells with ample amount of eosinophilic cytoplasm and prominent nucleoli. Numerous mitoses are identified.
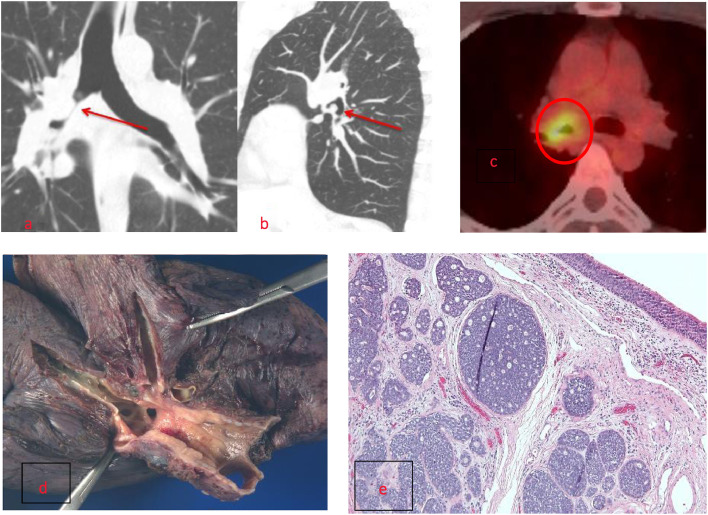
(a, b) Adenoid cystic carcinoma presenting as intraluminal mass within the proximal right main stem bronchus. Note the smooth contours and extent of longitudinal involvement that is longer than axial involvement as seen on coronal and sagittal CT imaging. (c) FDG PET-CT is demonstrating avid radiotracer uptake. (d, e) Gross pathology demonstrates ill-defined firm white-tan mass is enveloping the trachea measuring t 3.6 × 5 × 0.8 cm and extending into the right superior lobar bronchus. 10 X image with H&E staining demonstrates respiratory mucosa at the top with nests of ACC tumor cells below.
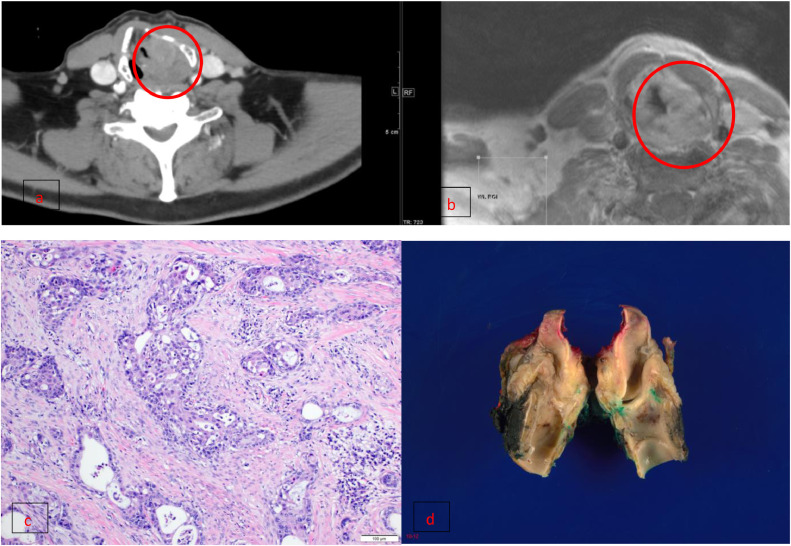
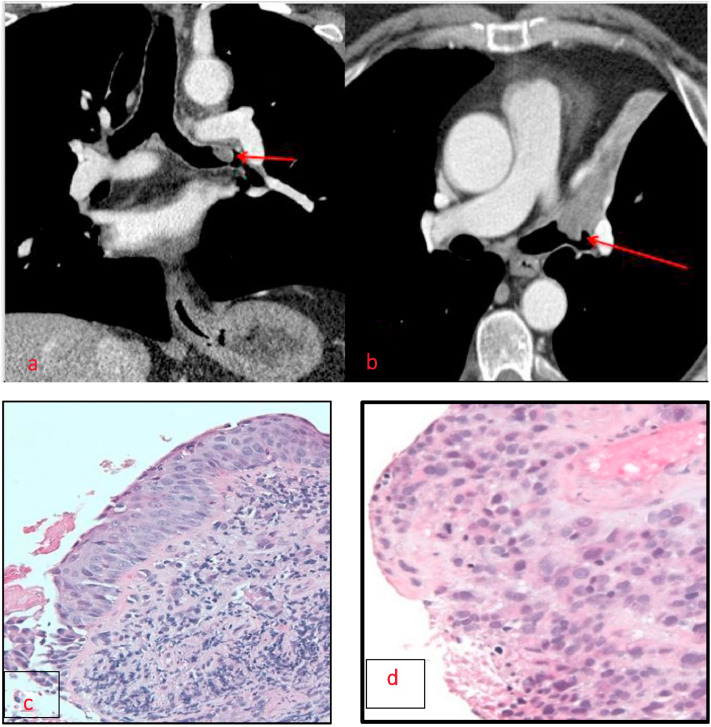
(a, b) Left glottic enhancing mass involving the left paraglottic fat and aryepiglottic fold. The mass infiltrates the true vocal cord and left cricothyroid space and abuts the left thyroid, arytenoid, and cricoid cartilages. Left: Contrast-enhanced neck CT, Right: Axial IDEAL T1 w/ contrast. (c, d) Sections demonstrate sheets and nests of infiltrating tumor cells characterized by enlarged, pleomorphic nuclei with ample amounts of eosinophilic cytoplasm with extensive microcystic and cribiforming architectures. Overall the features are diagnostic of intermediate-grade mucoepidermoid carcinoma.
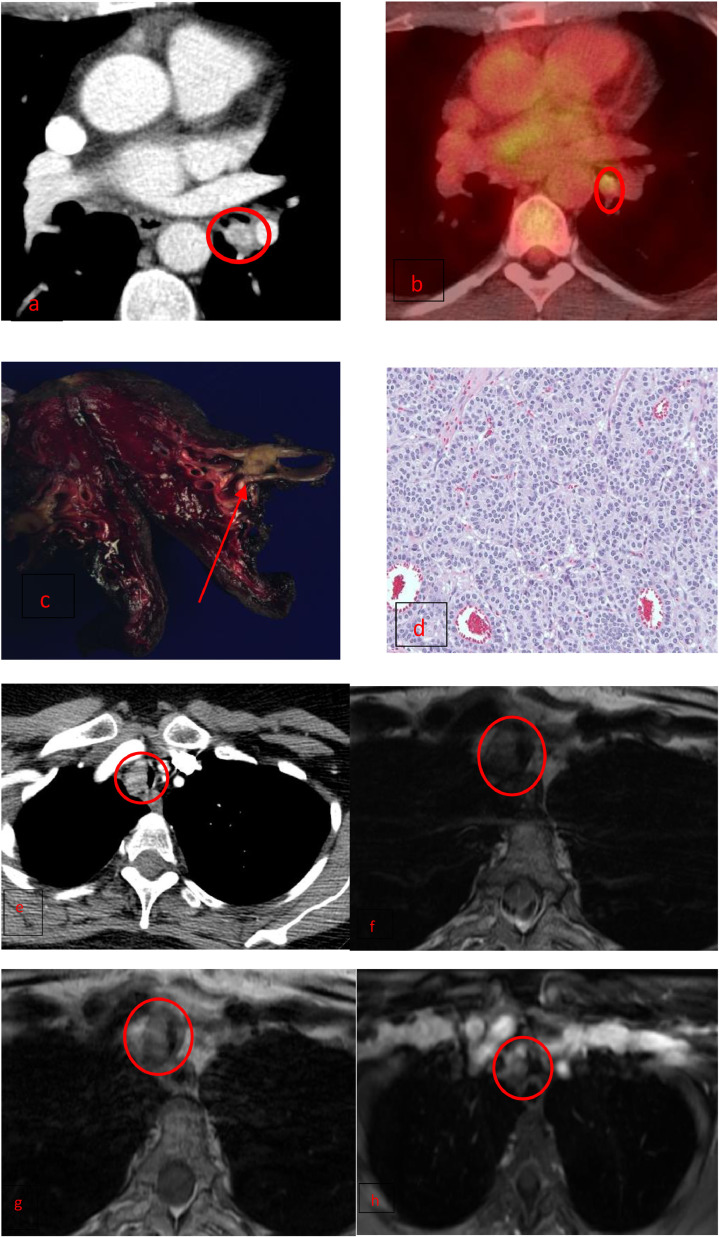
(a) Endobronchial carcinoid visualized as an enhancing, well-defined ovoid nodule arising from the left lower lobar bronchus. (b) Carcinoid is demonstrating low FDG avidity on PET/CT. (c) Gross pathology is demonstrating a 1.6 × 1.0 × 1.0 cm well circumscribed, endobronchial, tan-white nodule arising from the left lower lobe bronchus, within 0.5 cm of the inked specimen edge, and 0.5 cm to the inked bronchial specimen edge. (d) 20 X H&E stain showing small nests of uniform cells representing a typical carcinoid. (e-h) Partial obstruction of the mid trachea by an enhancing mass which is mild hyperintense on T2 (f) and isointense on T1(g). The lesion is avidly enhancing with contrast. This mass was found to be a cardinoid.
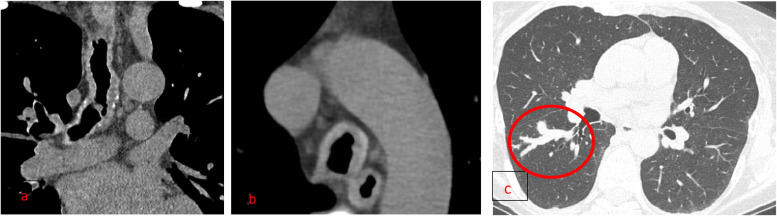
(a, b) Endobronchial lymphoma is manifesting as a large intraluminal mass expanding the right main bronchus and extending into the bronchus intermedius. (c) FDG PET is showing intense uptake corresponding to the intraluminal soft tissue mass and subcarinal lymphadenopathy. (d) H&E stained sections show bronchial mucosa with a lymphoid infiltrate expanding the submucosa, composed of predominantly small sized cells with condensed chromatin and irregular nuclei. The findings are consistent with bronchial involvement by non-Hodgkin's lymphoma.
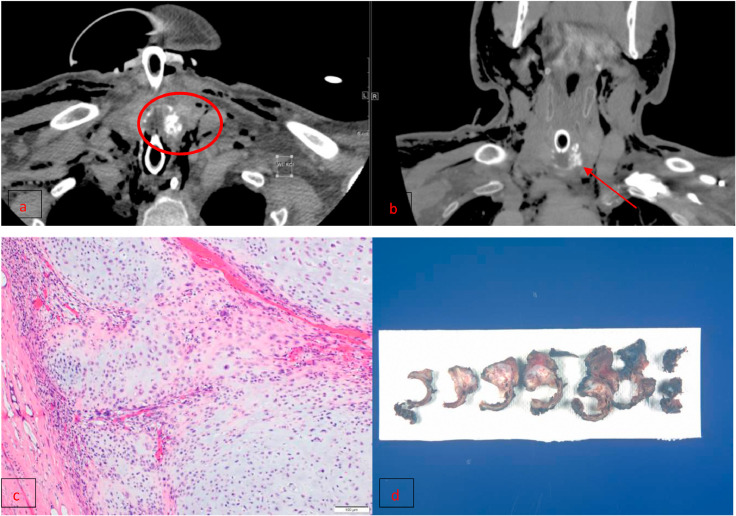
(a, b) CT in the axial (left) and coronal planes (right) demonstrates a laryngopharyngeal mass with abnormal soft tissue and internal irregular calcifications consistent with chondroid matrix eroding the left aspect of the upper trachea. This mass extends into the postcricoid larynx and glottic larynx. Tracheostomy cannula and post-tracheostomy pneuma-mediastinum and subcutaneous emphysema are also demonstrated. (c, d) Portions of the current resection specimen show chondrosarcoma with foci of low-grade cellularity (grade 1).
(a, b) Enhancing nodule in the left main bronchus producing the partial collapse of the left upper lobe in a patient with a known history of melanoma. (c) Fragment of respiratory mucosa. (d) Fragment of metastatic melanoma.
(a, b) Diffuse tracheal wall thickening with mild nodularity without calcification is compatible with Rhinoscleroma. (c) Mucoid impaction within the lobar bronchus (finger in glove sign), which can be seen in airways infection and ABPA. Such as Aspergillosis.
(a, b) Diffuse tracheal wall thickening producing bronchial stenosis. (c) Acute and chronic inflammation, follicular bronchiolitis, dense interstitial lymphoplasmacytic infiltrate, and blood vessels with granulomatous inflammation and fibrosis.
(a) Multiple partially calcified soft tissue nodules in the trachea, with the involvement of the posterior membrane as seen on sagittal view. (b) Low magnification image demonstrates eosinophilic amorphous material compatible with amyloid deposition.
Diffuse smooth tracheal wall thickening is sparing the posterior wall in a patient with relapsing polychondritis.
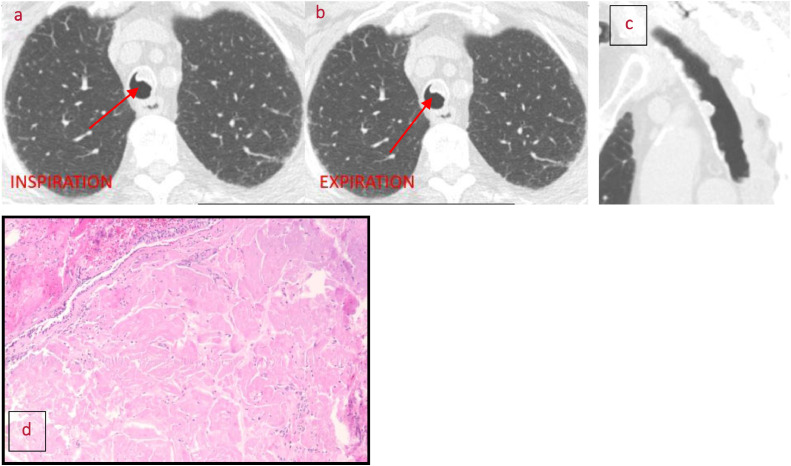
Endoluminal nodules in the trachea with thin-walled cysts and nodules in the lung parenchyma reflecting respiratory papillomatosis.
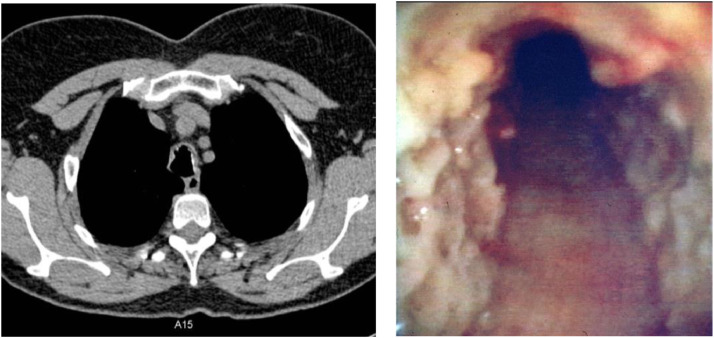
Osteocartilaginous nodules are sparing the posterior trachea reflecting Tracheobronchopathia Osteochondroplastica (TPO) with a bronchoscopic view of the trachea (Image courtesy of Justus Roos, MD).
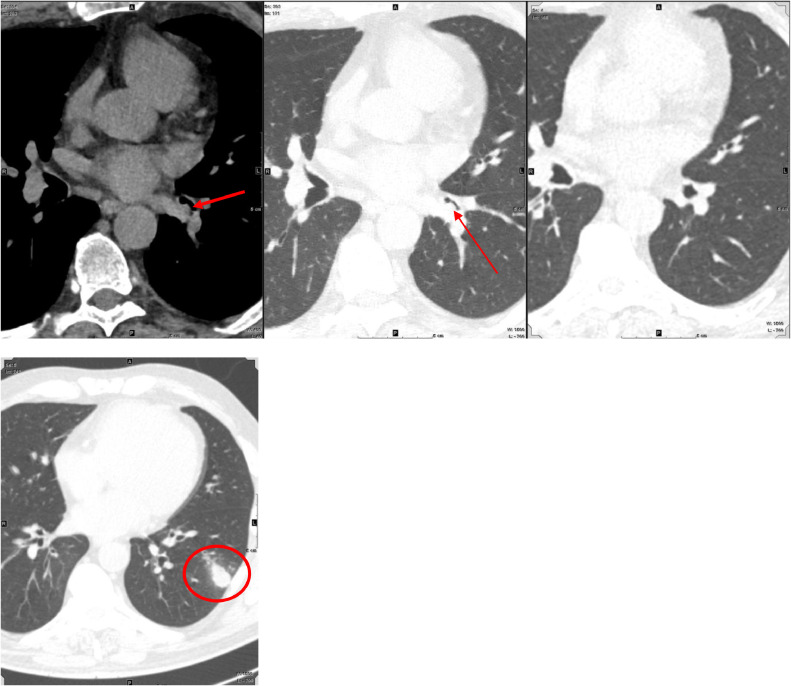
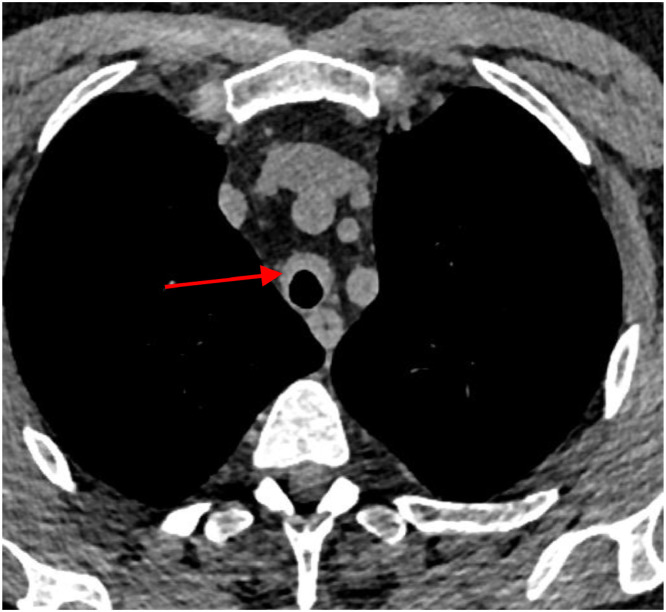
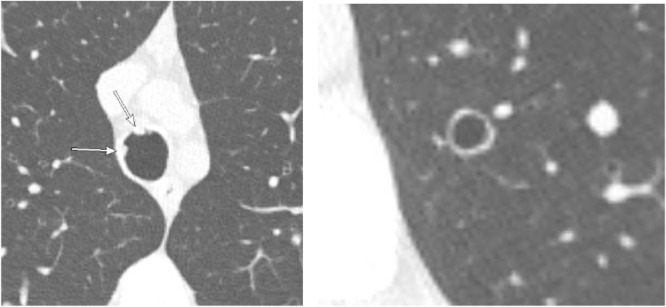
(From left to right) 65-year-old man with cough lasting several weeks. An endoluminal lesion at the origin of the left lower lobe basilar segmental bronchi was noted on CT at presentation (red arrows, A, mediastinal window; panel B, lung window). Bronchoscopy confirmed the presence of an aspirated peanut, which was removed and patency of the airway was restored (panel C). The patient developed a subsegmental area of aspiration pneumonia (image 2), which subsequently resolved on follow-up imaging (Image courtesy of Alex Bratt, MD). (Color version of figure is available online).
References
-
- Ngo A-VH, Walker CM, Chung JH, et al. Tumors and tumorlike conditions of the large airways. 2013;201:301-13. - PubMed
-
- Park CM, Goo JM, Lee HJ, et al. Tumors in the tracheobronchial tree: CT and FDG PET features. 2009;29:55-71. - PubMed
-
- Breatnach E., Abbott G.C., Fraser R.G. Dimensions of the normal human trachea. AJR Am J Roentgenol. 1984;142:903–906. - PubMed
-
- Hartman T.E., Primack S.L., Lee K.S. CT of bronchial and bronchiolar diseases. Radiographics. 1994;14:991–1003. - PubMed
-
- Holbert J.M., Strollo D.C. Imaging of the normal trachea. J Thorac Imaging. 1995;10:171–179. - PubMed
