

Leaky gut: mechanisms, measurement and clinical implications in humans
- PMID: 31076401
- PMCID: PMC6790068
- DOI: 10.1136/gutjnl-2019-318427
Leaky gut: mechanisms, measurement and clinical implications in humans
Abstract
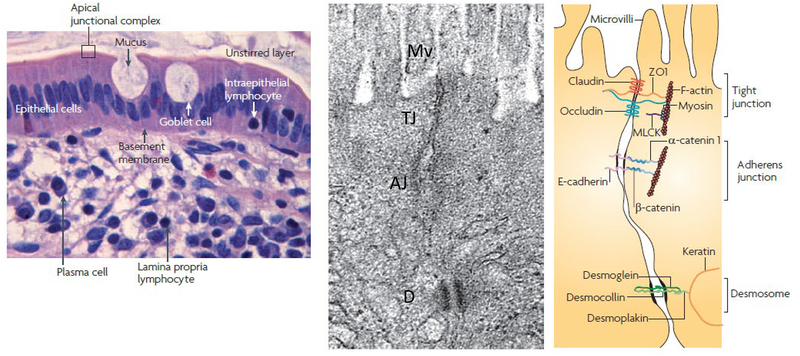
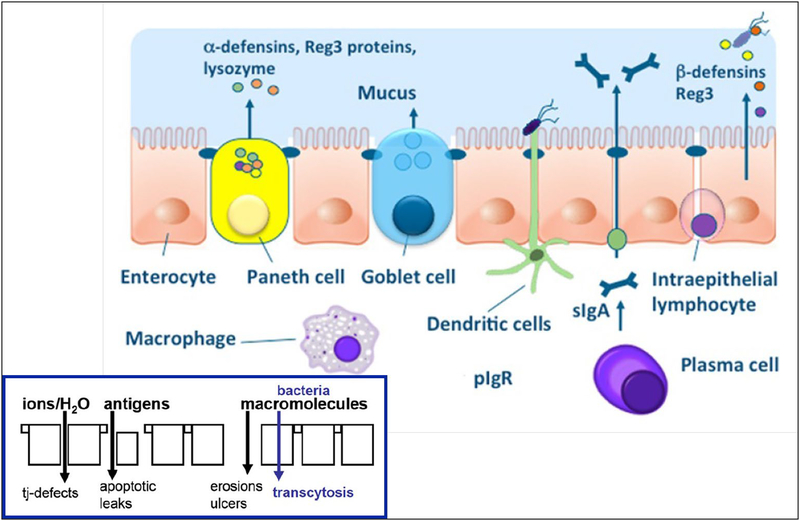
The objectives of this review on 'leaky gut' for clinicians are to discuss the components of the intestinal barrier, the diverse measurements of intestinal permeability, their perturbation in non-inflammatory 'stressed states' and the impact of treatment with dietary factors. Information on 'healthy' or 'leaky' gut in the public domain requires confirmation before endorsing dietary exclusions, replacement with non-irritating foods (such as fermented foods) or use of supplements to repair the damage. The intestinal barrier includes surface mucus, epithelial layer and immune defences. Epithelial permeability results from increased paracellular transport, apoptosis or transcellular permeability. Barrier function can be tested in vivo using orally administered probe molecules or in vitro using mucosal biopsies from humans, exposing the colonic mucosa from rats or mice or cell layers to extracts of colonic mucosa or stool from human patients. Assessment of intestinal barrier requires measurements beyond the epithelial layer. 'Stress' disorders such as endurance exercise, non-steroidal anti-inflammatory drugs administration, pregnancy and surfactants (such as bile acids and dietary factors such as emulsifiers) increase permeability. Dietary factors can reverse intestinal leakiness and mucosal damage in the 'stress' disorders. Whereas inflammatory or ulcerating intestinal diseases result in leaky gut, no such disease can be cured by simply normalising intestinal barrier function. It is still unproven that restoring barrier function can ameliorate clinical manifestations in GI or systemic diseases. Clinicians should be aware of the potential of barrier dysfunction in GI diseases and of the barrier as a target for future therapy.
Keywords: mucus; permeability; tight junctions.
© Author(s) (or their employer(s)) 2019. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Putative function of goblet cells as epithelial sealing in ischaemia/reperfusion-induced intestinal barrier dysfunction.Gut. 2020 Oct;69(10):1888-1890. doi: 10.1136/gutjnl-2019-319770. Epub 2019 Oct 30. Gut. 2020. PMID: 31666293 No abstract available.
References
-
- Chadwick VS, Phillips SF, Hofmann AF. Measurements of intestinal permeability using low molecular weight polyethylene glycols (PEG 400). II. Application to normal and abnormal permeability states in man and animals. Gastroenterology 1977;73:247–51. - PubMed
-
- Bjarnason I, Peters TJ, Veall N. A persistent defect in intestinal permeability in coeliac disease demonstrated by a 51Cr-labelled EDTA absorption test. Lancet 1983;1:323–5. - PubMed
-
- Hollander D, Vadheim CM, Brettholz E, et al. Increased intestinal permeability in Crohn’s patients and their relatives: an etiological factor. Ann Intern Med 1986;105:883–5. - PubMed
-
- Camilleri M, Vakil N. Microbiome: In search of mechanistic information and relevance. Am J Gastroenterol (submitted) - PubMed
-
- Maruvada P, Leone V, Kaplan LM, et al. The human microbiome and obesity: moving beyond associations. Cell Host Microbe 2017;22:589–99. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources