

Physical activity and dietary interventions in diabetic neuropathy: a systematic review
- PMID: 31076938
- PMCID: PMC6697618
- DOI: 10.1007/s10286-019-00607-x
Physical activity and dietary interventions in diabetic neuropathy: a systematic review
Abstract
Purpose: Diabetic neuropathy is a common and disabling disorder, and there are currently no proven effective disease-modifying treatments. Physical activity and dietary interventions in patients with diabetes and diabetic neuropathy have multiple beneficial effects and are generally low risk, which makes lifestyle interventions an attractive treatment option. We reviewed the literature on the effects of physical activity and dietary interventions on length-dependent peripheral neuropathy and cardiac autonomic neuropathy in diabetes.
Methods: The electronic database PubMed was systematically searched for original human and mouse model studies examining the effect of either dietary or physical activity interventions in subjects with diabetes, prediabetes, or metabolic syndrome.
Results: Twenty studies are included in this review. Fourteen studies were human studies and six were in mice. Studies were generally small with few controlled trials, and there are no widely agreed upon outcome measures.
Conclusions: Recent research indicates that dietary interventions are effective in modifying diabetic neuropathy in animal models, and there are promising data that they may also ameliorate diabetic neuropathy in humans. It has been known for some time that lifestyle interventions can prevent the development of diabetic neuropathy in type 2 diabetes mellitus subjects. However, there is emerging evidence that lifestyle interventions are effective in individuals with established diabetic neuropathy. In addition to the observed clinical value of lifestyle interventions, there is emerging evidence of effects on biochemical pathways that improve muscle function and affect other organ systems, including the peripheral nerve. However, data from randomized controlled trials are needed.
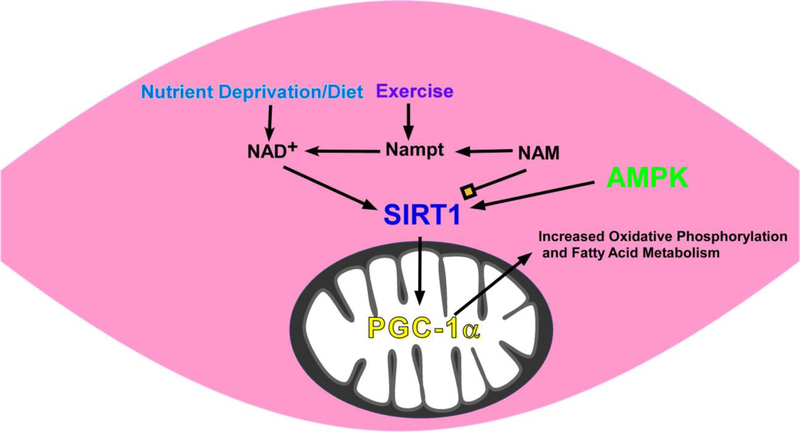
Keywords: Diabetic neuropathy; Diet; Dysautonomia; Exercise; Sirtuins.
Figures
References
-
- UKPDS (1998) Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet 352:837–853 - PubMed
-
- American Diabetes A (2018) 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2018. Diabetes Care 41:S13–S27 - PubMed
-
- Ametov AS, Barinov A, Dyck PJ, Hermann R, Kozlova N, Litchy WJ, Low PA, Nehrdich D, Novosadova M, O’Brien PC, Reljanovic M, Samigullin R, Schuette K, Strokov I, Tritschler HJ, Wessel K, Yakhno N, Ziegler D (2003) The sensory symptoms of diabetic polyneuropathy are improved with a-lipoic acid: The Sydney trial. Diabetes Care 26:770–776 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
