

Morphological analysis for subaxial cervical pedicle screw insertion in developmental and non-developmental canal stenosis
- PMID: 31077170
- PMCID: PMC6511180
- DOI: 10.1186/s12891-019-2577-1
Morphological analysis for subaxial cervical pedicle screw insertion in developmental and non-developmental canal stenosis
Abstract
Background: This study aimed to evaluate the safety and feasibility of subaxial cervical pedicle screw (CPS) insertion by comparing the morphological parameters between developmental canal stenosis (DCS) and non-developmental canal stenosis (NDCS) patients.
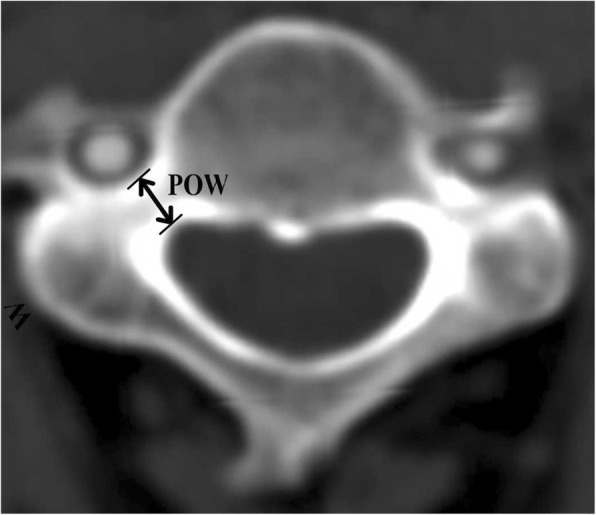
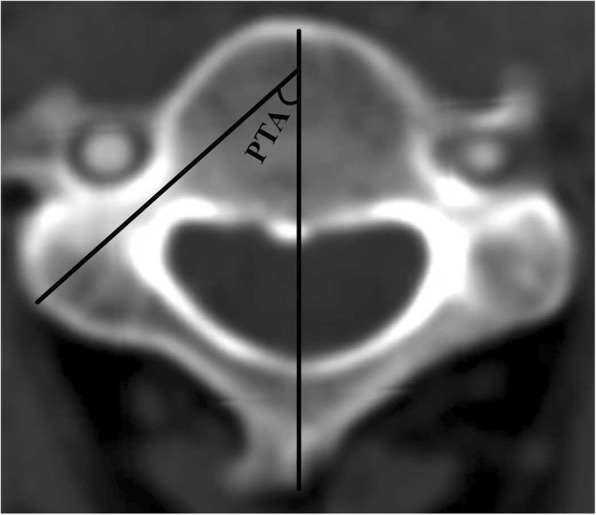
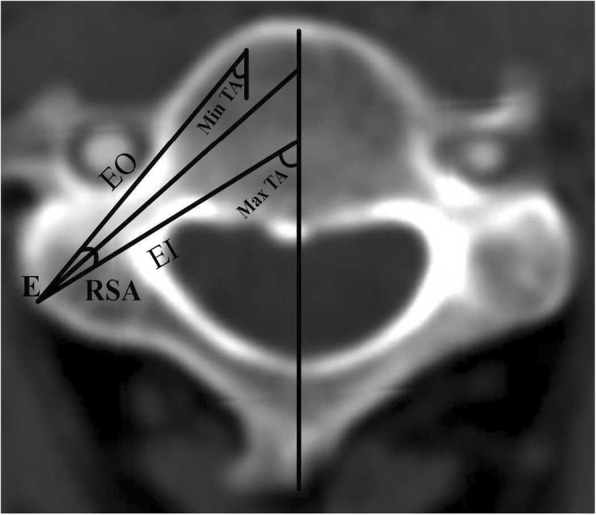
Methods: A total of 120 Chinese patients who had undergone cervical spinal multiplanar CT imaging from September 2010 to December 2014 were included in this study. According to the Pavlov ratio (PR), participants were classified into a DCS group (PR < 0.82) and an NDCS group (PR ≥0.82). CT reconstruction images of the cervical pedicles from C3 to C7 were selected for further analysis, and detailed morphological parameters for subaxial CPS insertion including pedicle outer width (POW), tiny cervical pedicle (TCP), pedicle transverse angle (PTA), and range of safe angle (RSA) were measured and compared in these two groups.
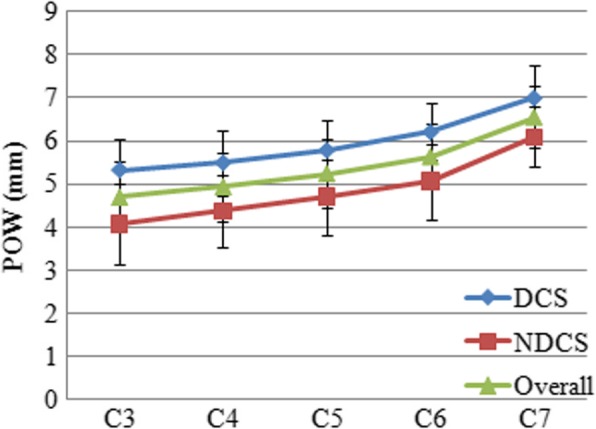
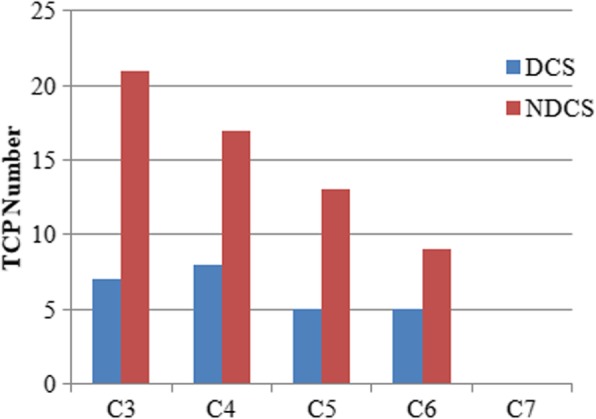
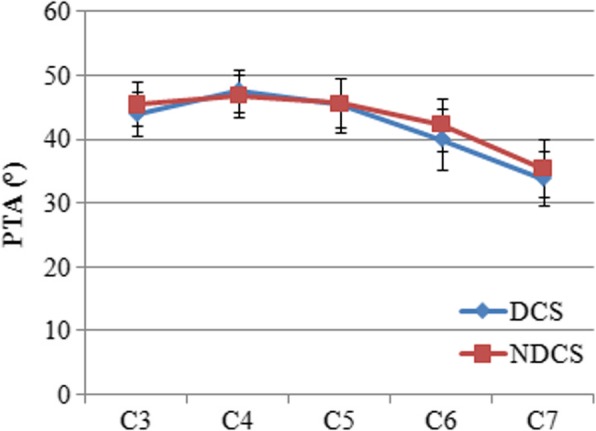
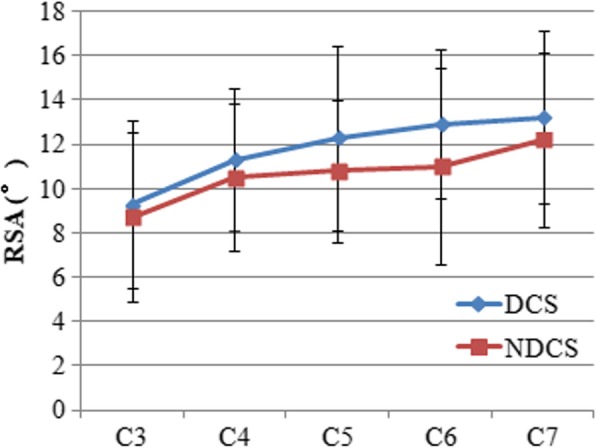
Results: A total of 600 images (1200 pedicles) from these 120 patients were measured. The POW in the DCS group was wider than that in the NDCS group at each level, while the number of TCPs in the DCS group was significantly less than that in the NDCS group at the C3, C4, and C5 vertebrae. There was no significant difference in PTA at any level between the two groups, however the RSA in the DCS group was greater than that in the NDCS group from C4 to C7.
Conclusions: Subaxial CPS for DCS patients may be safer and more feasible than that for NDCS patients. However, as the subaxial cervical pedicle is relatively small, CPS insertion is difficult and preoperative CT evaluation is recommended for both DCS and NDCS patients.
Keywords: Computed tomography; Developmental canal stenosis; Parameter; Pedicle morphology; Pedicle screw; Subaxial cervical spine.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the ethics committee of The Affiliated Hospital of Southwest Medical University. All patients provided written informed consent prior to their inclusion in this study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Morphological analysis of the cervical pedicles, lateral masses, and laminae in developmental canal stenosis.Spine (Phila Pa 1976). 2010 Nov 15;35(24):E1381-5. doi: 10.1097/BRS.0b013e3181e8958f. Spine (Phila Pa 1976). 2010. PMID: 21030896
-
Cervical pedicle screw placement: feasibility and accuracy of two new insertion techniques based on morphometric data.Eur Spine J. 2007 Jan;16(1):47-56. doi: 10.1007/s00586-006-0104-1. Epub 2006 Apr 21. Eur Spine J. 2007. PMID: 16628443 Free PMC article.
-
The "slide technique"-a novel free-hand method of subaxial cervical pedicle screw placement.BMC Musculoskelet Disord. 2020 Jun 23;21(1):399. doi: 10.1186/s12891-020-03420-0. BMC Musculoskelet Disord. 2020. PMID: 32576178 Free PMC article.
-
Ethnic differences in pedicle and bony spinal canal dimensions calculated from computed tomography of the cervical spine: a review of the English-language literature.Eur Spine J. 2012 Aug;21(8):1451-8. doi: 10.1007/s00586-012-2295-y. Epub 2012 Apr 19. Eur Spine J. 2012. PMID: 22526698 Free PMC article. Review.
-
Accuracy and safety assessment of subaxial cervical pedicle screw instrumentation: a systematic review.Spine J. 2025 May 5:S1529-9430(25)00237-2. doi: 10.1016/j.spinee.2025.05.006. Online ahead of print. Spine J. 2025. PMID: 40334991 Review.
Cited by
-
CT correlation of spinal canal diameter with pedicle size for safer posterior cervical pedicle screw fixation.Surg Neurol Int. 2024 Aug 30;15:307. doi: 10.25259/SNI_590_2024. eCollection 2024. Surg Neurol Int. 2024. PMID: 39246797 Free PMC article.
References
-
- Nakashima H, Yukawa Y, Suda K, Yamagata M, Ueta T, Kato F. Relatively large cervical spinal cord for Spinal Canal is a risk factor for development of cervical spinal cord compression: a cross-sectional study of 1211 subjects. Spine. 2016;41:E342–E348. doi: 10.1097/BRS.0000000000001255. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
