

Peripheral adenomatoid odontogenic tumor in a cloak of an epulis: report of a rare case
- PMID: 31077195
- PMCID: PMC6511215
- DOI: 10.1186/s12903-019-0759-8
Peripheral adenomatoid odontogenic tumor in a cloak of an epulis: report of a rare case
Abstract
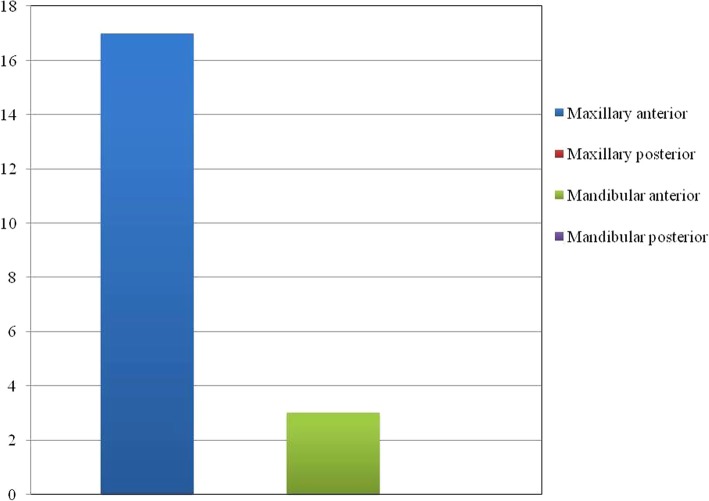
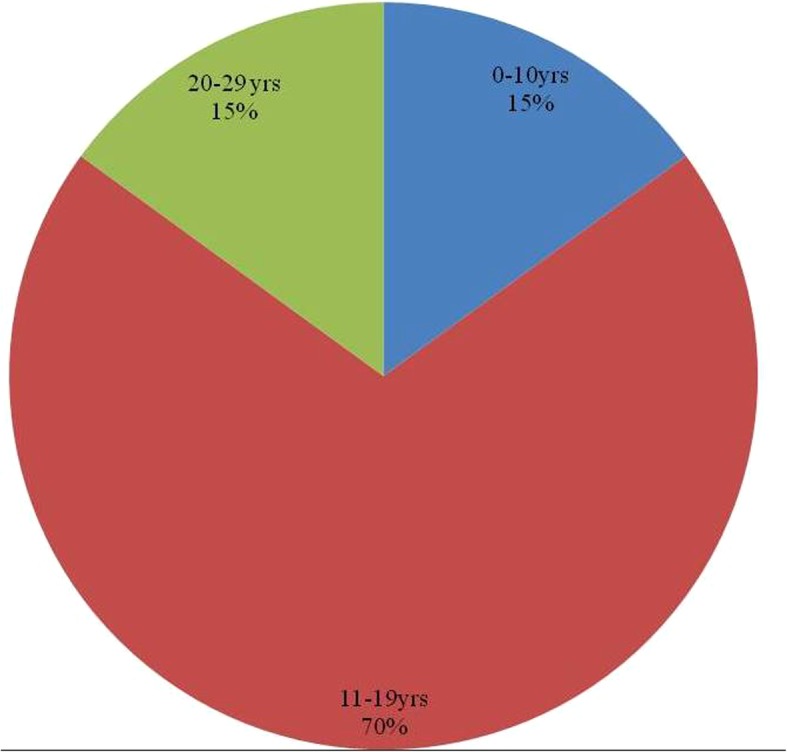
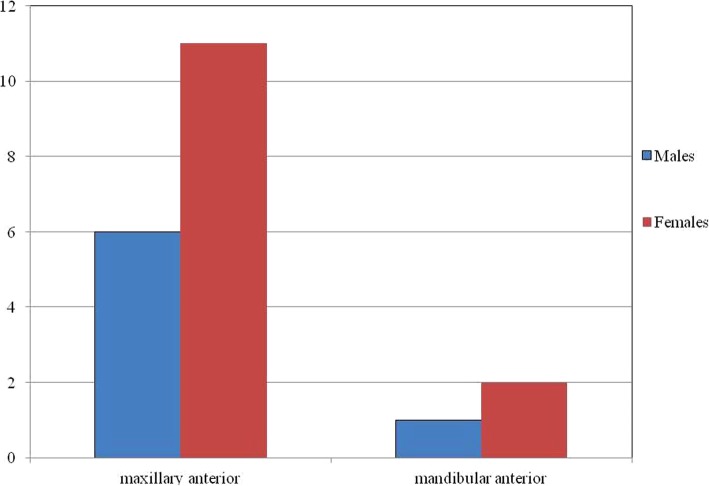
Background: Adenomatoid odontogenic tumor constitutes an uncommon benign odontogenic tumor which is well-known as "two-thirds tumor" (two-thirds of adenomatoid tumors occur in the maxilla, two-thirds occur in young females, two-thirds of the cases are associated with un-erupted teeth and two-thirds of the affected teeth are canines). Larger part of these present as intra - osseous tumors while peripheral counterparts are extremely rare. Peripheral adenomatoid odontogenic tumor is a unique entity which generally presents as a slow growing gingival swelling with minimal bone involvement. This often leads to its erroneous diagnosis as a simple gingival lesion and the real diagnosis is only revealed after its microscopic evaluation. It exhibits a marked predilection for maxillary gingiva of incisor region and most commonly affects the younger females.
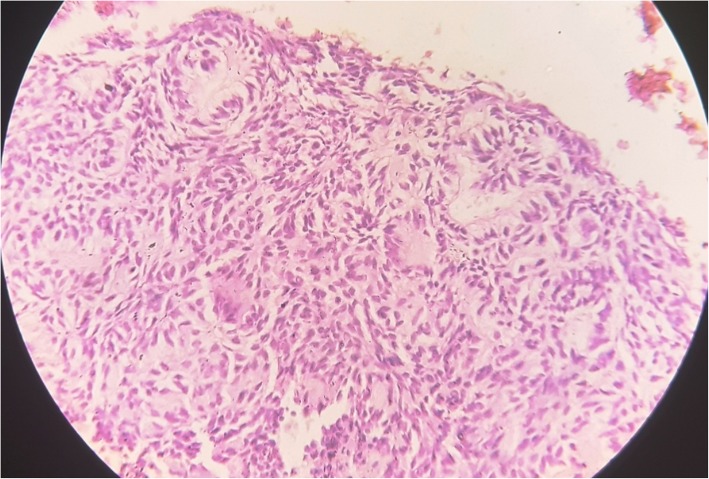
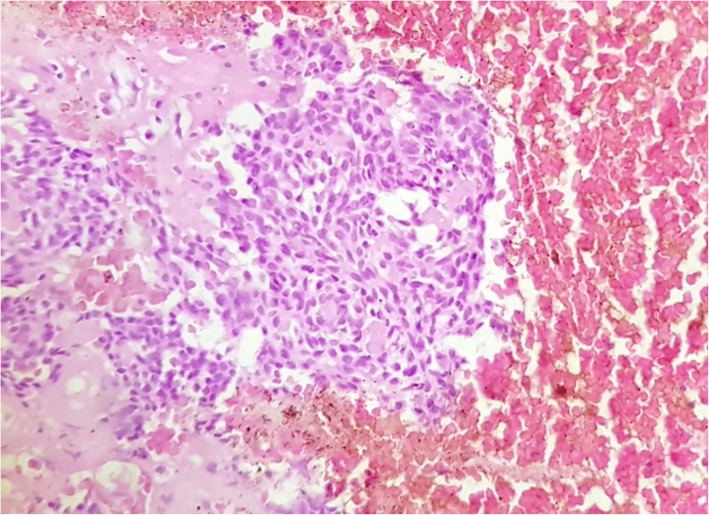
Case presentation: We report a case of 25 years old female patient of African ethnicity who presented with a 2 × 2 cm mass attached to the left mandibular gingiva in cuspid- bicuspid region which is an unusual site for AOT. It was accompanied by slight bone loss. With the differential diagnosis of gingival epulis and peripheral ossifying fibroma; surgical excision was performed. The light microscopic examination of the specimen aided the final diagnosis of Adenomatoid odontogenic tumor with the histopathological features identical to its intra osseous counterpart.
Conclusion: In this case, the tumor is present on the mandibular gingiva in a 25 years old patient which is an atypical location and age for this tumor; also, the only individual case reported in an African patient. Only, a meager number of peripheral adenomatoid odontogenic tumor cases have been logged so far with majority of them occurring in maxillary gingiva. Furthermore, an ambiguity still prevails regarding its true origin and possible biological course. Hence, reporting of similar cases should be encouraged to facilitate the better understanding of its varied epidemiological details and clinical presentation.
Keywords: Adenomatoid odontogenic tumor; Gingival lesions; Peripheral adenomatoid odontogenic tumor; Peripheral odontogenic tumors.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable
Consent for publication
Written informed consent was obtained from the patient for publication of this case report.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Lucas R. Pathology of tumours of the oral tissues. 4. Edinburgh: Churchill Livingstone; 1984. pp. 61–66.
-
- Pindborg JJ, Kramer IRH. WHO histological typing of odontogenic tumours, jaw cysts and allied lesions. 1. Geneva: Springer-Verlag; 1971.
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
