

Effect and safety of treatment with ACE-inhibitor Enalapril and β-blocker metoprolol on the onset of left ventricular dysfunction in Duchenne muscular dystrophy - a randomized, double-blind, placebo-controlled trial
- PMID: 31077250
- PMCID: PMC6509833
- DOI: 10.1186/s13023-019-1066-9
Effect and safety of treatment with ACE-inhibitor Enalapril and β-blocker metoprolol on the onset of left ventricular dysfunction in Duchenne muscular dystrophy - a randomized, double-blind, placebo-controlled trial
Abstract
Background: X-linked Duchenne muscular dystrophy (DMD), the most frequent human hereditary skeletal muscle myopathy, inevitably leads to progressive dilated cardiomyopathy. We assessed the effect and safety of a combined treatment with the ACE-inhibitor enalapril and the β-blocker metoprolol in a German cohort of infantile and juvenile DMD patients with preserved left ventricular function.
Methods trial design: Sixteen weeks single-arm open run-in therapy with enalapril and metoprolol followed by a two-arm 1:1 randomized double-blind placebo-controlled treatment in a multicenter setting.
Inclusion criteria: DMD boys aged 10-14 years with left ventricular fractional shortening [LV-FS] ≥ 30% in echocardiography. Primary endpoint: time from randomization to first occurrence of LV-FS < 28%. Secondary: changes of a) LV-FS from baseline, b) blood pressure, c), heart rate and autonomic function in ECG and Holter-ECG, e) cardiac biomarkers and neurohumeral serum parameters, f) quality of life, and g) adverse events.
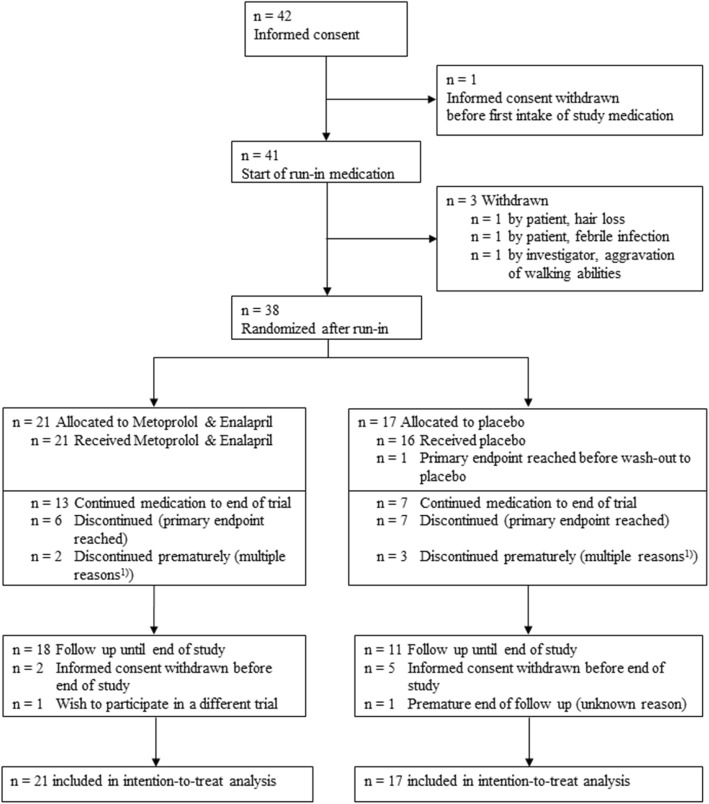
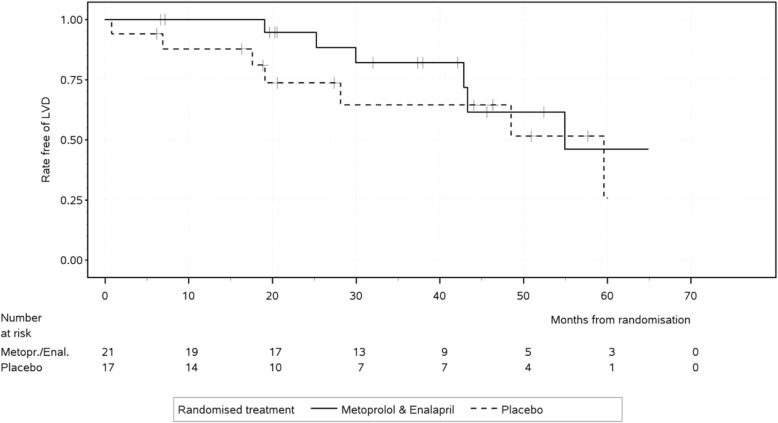
Results: From 3/2010 to 12/2013, 38 patients from 10 sites were centrally randomized after run-in, with 21 patients continuing enalapril and metoprolol medication and 17 patients receiving placebo. Until end of study 12/2015, LV-FS < 28% was reached in 6/21 versus 7/17 patients. Cox regression adjusted for LV-FS after run-in showed a statistically non-significant benefit for medication over placebo (hazard ratio: 0.38; 95% confidence interval: 0.12 to 1.22; p = 0.10). Analysis of secondary outcome measures revealed a time-dependent deterioration of LV-FS with no statistically significant differences between the two study arms. Blood pressure, maximal heart rate and mean-NN values were significantly lower at the end of open run-in treatment compared to baseline. Outcome analysis 19 months after randomization displayed significantly lower maximum heart rate and higher noradrenalin and renin values in the intervention group. No difference between treatments was seen for quality of life. As a single, yet important adverse event, the reversible deterioration of walking abilities of one DMD patient during the run-in period was observed.
Conclusions: Our analysis of enalapril and metoprolol treatment in DMD patients with preserved left ventricular function is suggestive to delay the progression of the intrinsic cardiomyopathy to left ventricular failure, but did not reach statistical significance, probably due to insufficient sample size.
Clinical trial registration: DRKS-number 00000115, EudraCT-number 2009-009871-36.
Keywords: ACE-inhibitors; Cardiomyopathy; Duchenne muscular dystrophy; ß-blockers.
Conflict of interest statement
Ethics approval and consent to participate
Ethics approval was obtained from the ethics-committee of the medical faculty of the Friedrich-Alexander-Universität Erlangen-Nürnberg (protocol No. 2009–009871-36); informed consent was obtained from all participants and their parents.
Consent for publication
not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Bladen CL, Salgado D, Monges S, Foncuberta ME, Kekou K, Kosma K, Dawkins H, Lamont L, Roy AJ, Chamova T, Guergueltcheva V, Chan S, Korngut L, Campbell C, Dai Y, Wang J, Barisic N, Brabec P, Lahdetie J, Walter MC, Schreiber-Katz O, Karcagi V, Garami M, Viswanathan V, Bayat F, Buccella F, Kimura E, Koeks Z, van den Bergen JC, Rodrigues M, Roxburgh R, Lusakowska A, Kostera-Pruszczyk A, Zimowski J, Santos R, Neagu E, Artemieva S, Rasic VM, Vojinovic D, Posada M, Bloetzer C, Jeannet PY, Joncourt F, Diaz-Manera J, Gallardo E, Karaduman AA, Topaloglu H, El Sherif R, Stringer A, Shatillo AV, Martin AS, Peay HL, Bellgard MI, Kirschner J, Flanigan KM, Straub V, Bushby K, Verschuuren J, Aartsma-Rus A, Beroud C, Lochmuller H. The TREAT-NMD DMD global database: analysis of more than 7,000 Duchenne muscular dystrophy mutations. Hum Mutat. 2015;36:395–402. doi: 10.1002/humu.22758. - DOI - PMC - PubMed
-
- Bushby K, Finkel R, Birnkrant DJ, Case LE, Clemens PR, Cripe L, Kaul A, Kinnett K, McDonald C, Pandya S, Poysky J, Shapiro F, Tomezsko J, Constantin C, Group DMDCCW Diagnosis and management of Duchenne muscular dystrophy, part 1: diagnosis, and pharmacological and psychosocial management. Lancet Neurol. 2010;9:77–93. doi: 10.1016/S1474-4422(09)70271-6. - DOI - PubMed
-
- Bonnemann CG, Wang CH, Quijano-Roy S, Deconinck N, Bertini E, Ferreiro A, Muntoni F, Sewry C, Beroud C, Mathews KD, Moore SA, Bellini J, Rutkowski A, North KN. Diagnostic approach to the congenital muscular dystrophies. Neuromuscul Disord. 2014;24:289–311. doi: 10.1016/j.nmd.2013.12.011. - DOI - PMC - PubMed
-
- Raman SV, Hor KN, Mazur W, Halnon NJ, Kissel JT, He X, Tran T, Smart S, McCarthy B, Taylor MD, Jefferies JL, Rafael-Fortney JA, Lowe J, Roble SL, Cripe LH. Eplerenone for early cardiomyopathy in Duchenne muscular dystrophy: a randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2015;14:153–161. doi: 10.1016/S1474-4422(14)70318-7. - DOI - PMC - PubMed
-
- Dittrich S, Tuerk M, Haaker G, Greim V, Buchholz A, Burkhardt B, Fujak A, Trollmann R, Schmid A, Schroeder R. Cardiomyopathy in Duchenne muscular dystrophy: current value of clinical, electrophysiological and imaging findings in children and teenagers. Klinische Padiatrie. 2015;227:225–231. doi: 10.1055/s-0034-1398689. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous
