

Automated treatment planning of postmastectomy radiotherapy
- PMID: 31077593
- PMCID: PMC6739169
- DOI: 10.1002/mp.13586
Automated treatment planning of postmastectomy radiotherapy
Abstract
Purpose: Breast cancer is the most common cancer in women globally and radiation therapy is a cornerstone of its treatment. However, there is an enormous shortage of radiotherapy staff, especially in low- and middle-income countries. This shortage could be ameliorated through increased automation in the radiation treatment planning process, which may reduce the workload on radiotherapy staff and improve efficiency in preparing radiotherapy treatments for patients. To this end, we sought to create an automated treatment planning tool for postmastectomy radiotherapy (PMRT).
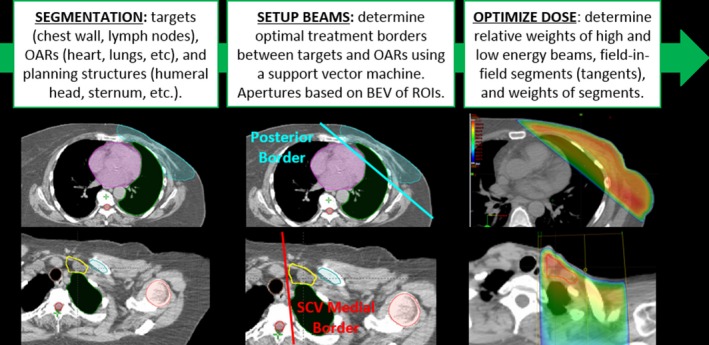
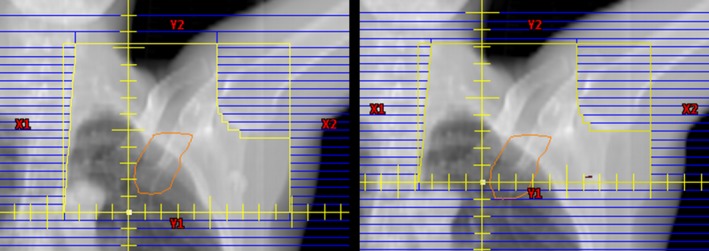
Methods: Algorithms to automate every step of PMRT planning were developed and integrated into a commercial treatment planning system. The only required inputs for automated PMRT planning are a planning computed tomography scan, a plan directive, and selection of the inferior border of the tangential fields. With no other human input, the planning tool automatically creates a treatment plan and presents it for review. The major automated steps are (a) segmentation of relevant structures (targets, normal tissues, and other planning structures), (b) setup of the beams (tangential fields matched with a supraclavicular field), and (c) optimization of the dose distribution by using a mix of high- and low-energy photon beams and field-in-field modulation for the tangential fields. This automated PMRT planning tool was tested with ten computed tomography scans of patients with breast cancer who had received irradiation of the left chest wall. These plans were assessed quantitatively using their dose distributions and were reviewed by two physicians who rated them on a three-tiered scale: use as is, minor changes, or major changes. The accuracy of the automated segmentation of the heart and ipsilateral lung was also assessed. Finally, a plan quality verification tool was tested to alert the user to any possible deviations in the quality of the automatically created treatment plans.
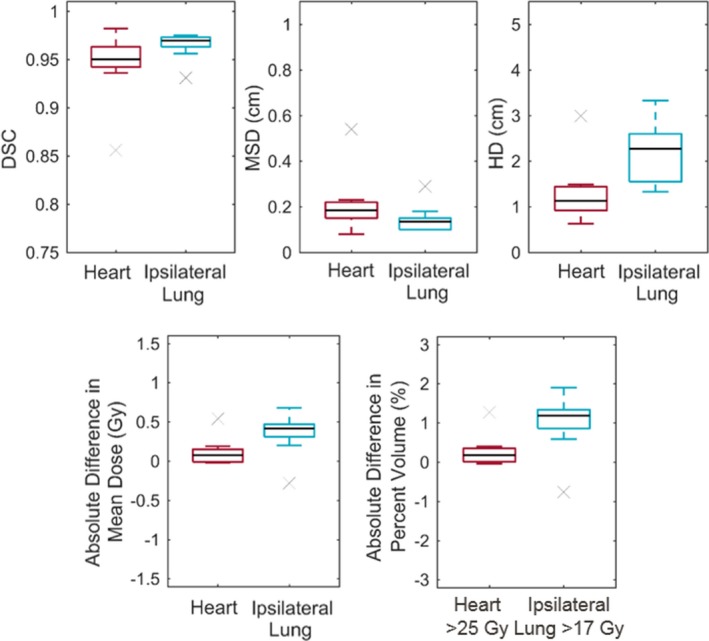
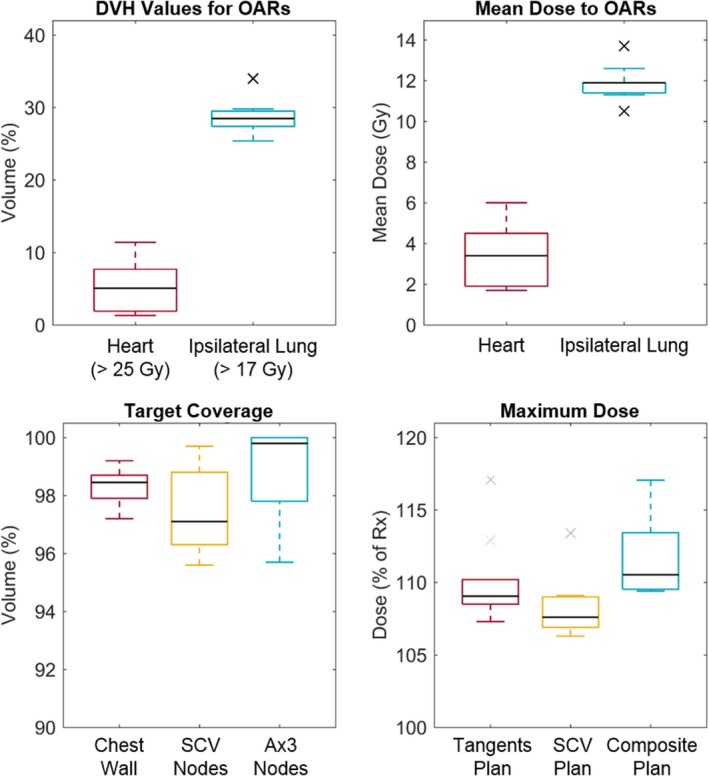
Results: The automatically created PMRT plans met the acceptable dose objectives, including target coverage, maximum plan dose, and dose to organs at risk, for all but one patient for whom the heart objectives were exceeded. Physicians accepted 50% of the treatment plans as is and required only minor changes for the remaining 50%, which included the one patient whose plan had a high heart dose. Furthermore, the automatically segmented contours of the heart and ipsilateral lung agreed well with manually edited contours. Finally, the automated plan quality verification tool detected 92% of the changes requested by physicians in this review.
Conclusions: We developed a new tool for automatically planning PMRT for breast cancer, including irradiation of the chest wall and ipsilateral lymph nodes (supraclavicular and level III axillary). In this initial testing, we found that the plans created by this tool are clinically viable, and the tool can alert the user to possible deviations in plan quality. The next step is to subject this tool to prospective testing, in which automatically planned treatments will be compared with manually planned treatments.
Keywords: automated treatment planning; postmastectomy radiotherapy.
© 2019 The Authors. Medical Physics published by Wiley Periodicals, Inc. on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
This work was partially supported by Varian Medical Systems.
Figures
References
-
- Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–E386. - PubMed
-
- Overgaard M, Jensen M‐B, Overgaard J, et al. Postoperative radiotherapy in high‐risk postmenopausal breast‐cancer patients given adjuvant tamoxifen: Danish Breast Cancer Cooperative Group DBCG 82c randomised trial. Lancet. 1999;353:1641–1648. - PubMed
-
- Overgaard M, Hansen PS, Overgaard J, et al. Postoperative radiotherapy in high‐risk premenopausal women with breast cancer who receive adjuvant chemotherapy. N Engl J Med. 1997;337:949–955. - PubMed
-
- Ragaz J, Olivotto IA, Spinelli JJ, et al. Locoregional radiation therapy in patients with high‐risk breast cancer receiving adjuvant chemotherapy: 20‐year results of the British Columbia randomized trial. J Natl Cancer Inst. 2005;97:116–126. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
