

Sparing Cardiac Substructures With Optimized Volumetric Modulated Arc Therapy and Intensity Modulated Proton Therapy in Thoracic Radiation for Locally Advanced Non-small Cell Lung Cancer
- PMID: 31077884
- PMCID: PMC6718306
- DOI: 10.1016/j.prro.2019.04.013
Sparing Cardiac Substructures With Optimized Volumetric Modulated Arc Therapy and Intensity Modulated Proton Therapy in Thoracic Radiation for Locally Advanced Non-small Cell Lung Cancer
Abstract
Purpose: Increasing radiation dose to the heart is associated with worse survival in stage III non-small cell lung cancer. We sought to evaluate the ability of optimized volumetric modulated arc therapy (VMAT) and intensity modulated proton therapy (IMPT) to spare cardiac substructures. We also wanted to determine how a cardiac optimization treatment planning algorithm influences dose distribution to other thoracic organs at risk (OARs).
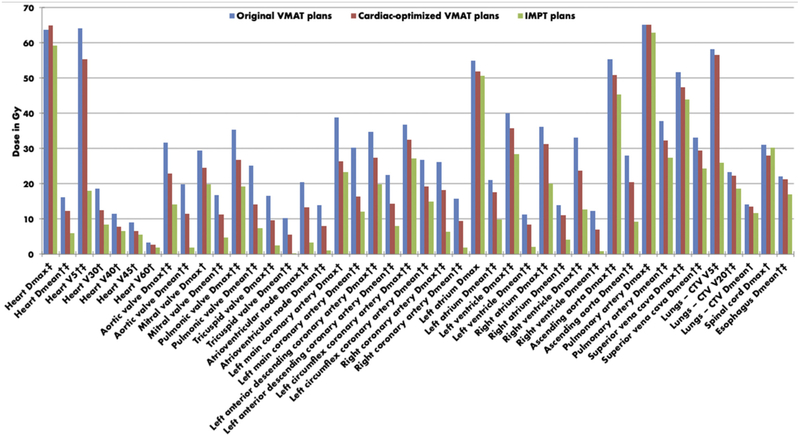
Methods and materials: Cardiac substructures were retrospectively contoured for all patients with stage III non-small cell lung cancer who were treated at our institution with VMAT to 60 Gy in 2-Gy fractions. The structures included valves, atrioventricular node, coronary arteries, chambers, and great vessels. New cardiac-optimized VMAT plans were created to spare these structures while preserving planning target volume coverage and maintaining standard dose constraints to OARs. Dosimetry variables for the new cardiac-optimized VMAT plans were compared via paired t test with the original VMAT plans. IMPT plans were also created, and the cardiac-optimized VMAT plans were then similarly compared with the IMPT plans.
Results: Twenty-six patients who were treated from July 2013 to September 2017 were included. Compared with the original VMAT plans, statistically significant improvements were demonstrated for all cardiac structures for the new cardiac-optimized VMAT plans while maintaining or improving appropriate lung, esophagus, and spinal cord constraints and planning target volume coverage goals. Compared with cardiac-optimized VMAT, IMPT demonstrated additional statistically significant improvements for some cardiac dosimetry metrics while maintaining or improving other thoracic OAR constraints.
Conclusions: VMAT is now widely available, and high-quality VMAT plans that incorporate cardiac substructures into the optimization process can provide overall improvements in dose to OARs and, in particular, substantial sparing of critical cardiac structures. IMPT provides some incremental dosimetric improvements beyond cardiac-optimized VMAT, the clinical significance of which remains uncertain.
Copyright © 2019 American Society for Radiation Oncology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Bradley JD, Paulus R, Komaki R, et al. Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): a randomised, two-by-two factorial phase 3 study. Lancet Oncol. 2015;16:187–199. - PMC - PubMed
-
- Speirs CK, DeWees TA, Rehman S, et al. Heart dose is an independent dosimetric predictor of overall survival in locally advanced non-small cell lung cancer. J Thorac Oncol. 2017;12:293–301. - PubMed
-
- Antonia SJ, Villegas A, Daniel D, et al. Overall survival with durvalumab after chemoradiotherapy in stage III NSCLC. N Engl J Med. 2018;379:2342–2350. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
