

Impact of disease progression on individual IPSS trajectories and consequences of immediate versus delayed start of treatment in patients with moderate or severe LUTS associated with BPH
- PMID: 31079189
- PMCID: PMC6994451
- DOI: 10.1007/s00345-019-02783-x
Impact of disease progression on individual IPSS trajectories and consequences of immediate versus delayed start of treatment in patients with moderate or severe LUTS associated with BPH
Abstract
Purpose: Despite superiority of tamsulosin-dutasteride combination therapy versus monotherapy for lower urinary tract symptoms due to benign prostatic hyperplasia (LUTS/BPH), patients at risk of disease progression are often initiated on α-blockers. This study evaluated the impact of initiating tamsulosin monotherapy prior to switching to tamsulosin-dutasteride combination therapy versus immediate combination therapy using a longitudinal model describing International Prostate Symptom Score (IPSS) trajectories in moderate/severe LUTS/BPH patients at risk of disease progression.
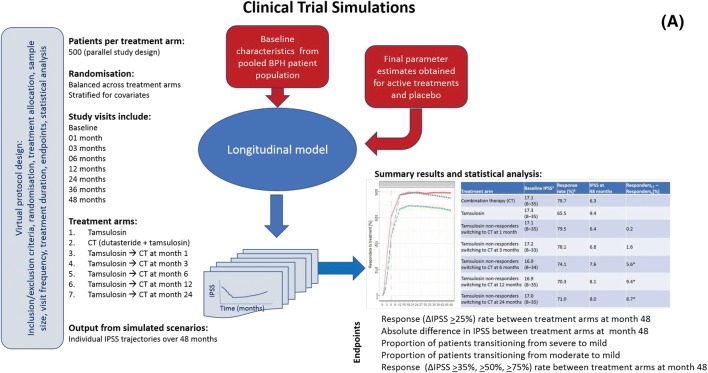
Methods: Clinical trial simulations (CTS) were performed using data from 10,238 patients from Phase III/IV dutasteride trials. The effect of varying disease progression rates was explored by comparing profiles on- and off-treatment. CTS scenarios were investigated, including a reference (immediate combination therapy) and six alternative virtual treatment arms (delayed combination therapy of 1-24 months). Clinical response (≥ 25% IPSS reduction relative to baseline) was analysed using log-rank test. Differences in IPSS relative to baseline at various on-treatment time points were assessed by t tests.
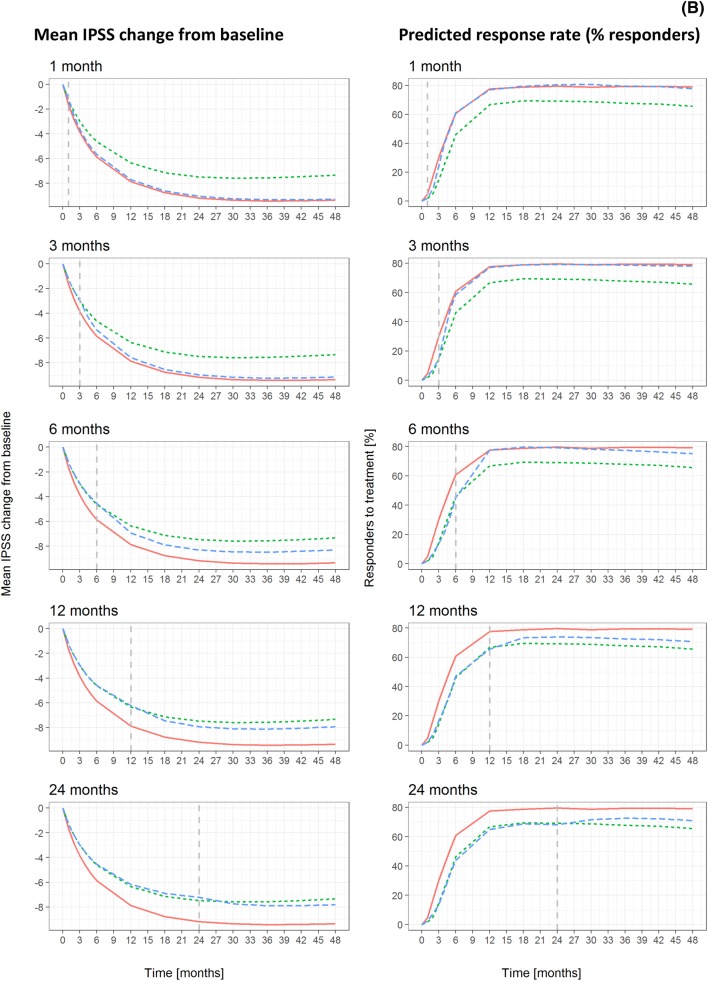
Results: Delayed combination therapy initiation led to significant (p < 0.01) decreases in clinical response. At month 48, clinical response rate was 79.7% versus 74.1%, 70.3% and 71.0% and IPSS was 6.3 versus 7.6, 8.1 and 8.0 (switchers from tamsulosin monotherapy after 6, 12 and 24 months, respectively) with immediate combination therapy. More patients transitioned from severe/moderate to mild severity scores by month 48.
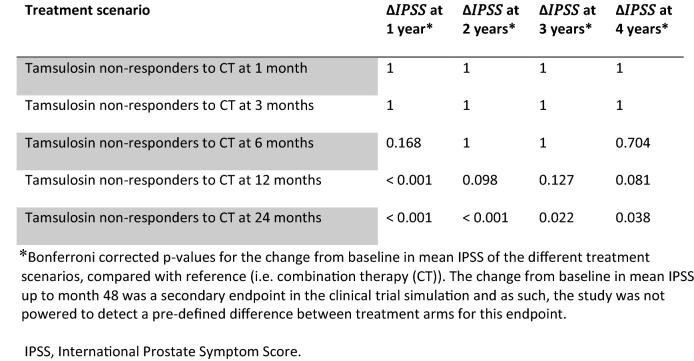
Conclusions: CTS allows systematic evaluation of immediate versus delayed combination therapy. Immediate response to α-blockers is not predictive of long-term symptom improvement. Observed IPSS differences between immediate and delayed combination therapy (6-24 months) are statistically significant.
Keywords: Benign prostatic hyperplasia; Clinical trial simulation; Drug–disease modelling; Dutasteride; Lower urinary tract symptoms; Tamsulosin.
Conflict of interest statement
SD has none to declare. TW holds stocks/shares in GSK. BA, MM, JMPM, CC and ODP are GSK employees and hold stocks/shares in GSK. MO has been a speaker, consultant and/or trial participant for Apogepha, Astellas, Duchesnay, Ferring, GSK, Lilly, Pierre Fabre and Pfizer, and received research grants from Astellas and Pfizer. CR was previously employed as a consultant to GSK.
Figures
Comment in
-
Benign Prostatic Hyperplasia.J Urol. 2021 Aug;206(2):447-450. doi: 10.1097/JU.0000000000001854. Epub 2021 May 14. J Urol. 2021. PMID: 33985341 No abstract available.
References
-
- Gravas S, Cornu JN, Drake MJ et al (2018) EAU guidelines on the management of non-neurogenic male lower urinary tract symptoms (LUTS), incl. benign prostatic obstruction (BPO). Available at: http://uroweb.org/guideline/treatment-of-non-neurogenic-male-luts/. Accessed 5 May 2019
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
