

Pharmacokinetics of adjusted-dose 8-hourly lopinavir/ritonavir in HIV-infected children co-treated with rifampicin
- PMID: 31081020
- PMCID: PMC6640304
- DOI: 10.1093/jac/dkz171
Pharmacokinetics of adjusted-dose 8-hourly lopinavir/ritonavir in HIV-infected children co-treated with rifampicin
Abstract
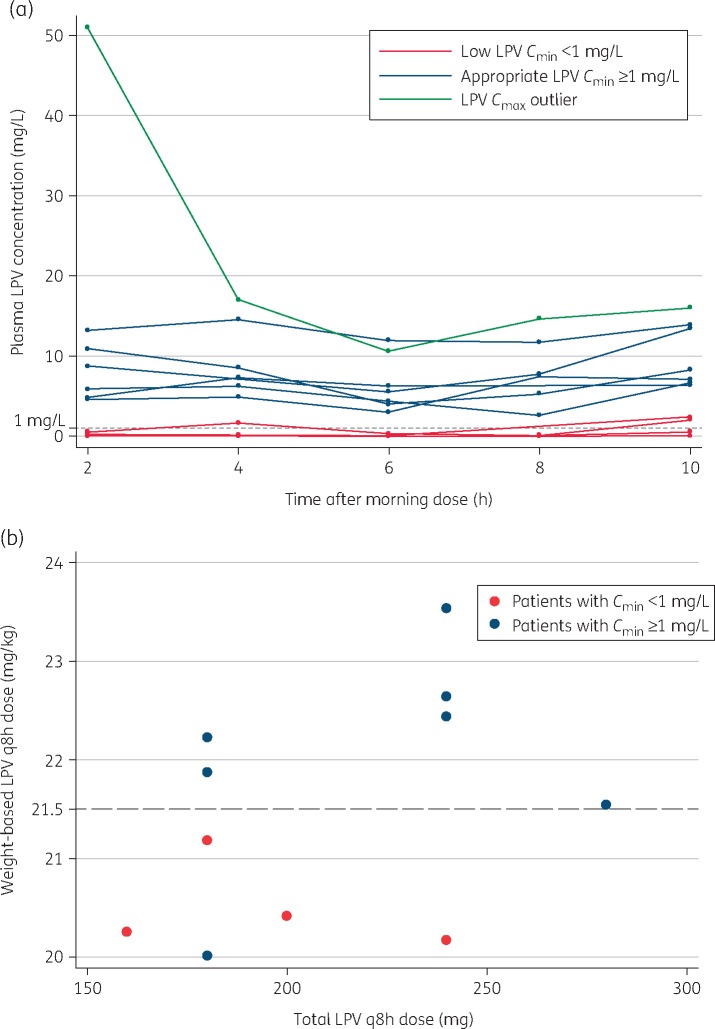
Objectives: To evaluate the proportion of children with lopinavir Cmin ≥1 mg/L when receiving a novel 8-hourly lopinavir/ritonavir dosing strategy during rifampicin co-treatment.
Methods: HIV-infected children on lopinavir/ritonavir and rifampicin were enrolled in a prospective pharmacokinetic study. Children were switched from standard-of-care lopinavir/ritonavir-4:1 with additional ritonavir (1:1 ratio) twice daily to 8-hourly lopinavir/ritonavir-4:1 using weight-banded dosing. Rifampicin was dosed at 10-20 mg/kg/day. After 2 weeks, plasma samples were collected ∼2, 4, 6, 8 and 10 h after the morning lopinavir/ritonavir-4:1 dose, ALT was obtained to assess safety and treatment was switched back to standard of care. ClinicalTrials.gov registration number: NCT01637558.
Results: We recruited 11 children in two weight bands: 5 (45%) were 10-13.9 kg and received 20-24 mg/kg/dose of lopinavir and 6 (55%) children weighed 6-9.9 kg and received 20-23 mg/kg/dose of lopinavir. The median age was 15 months (IQR = 12.6-28.8 months). The median (IQR) lopinavir Cmin was 3.0 (0.1-5.5) mg/L. Seven (63.6%) of the 11 children had Cmin values ≥1 mg/L. Children with a lopinavir mg/kg dose below the median 21.5 were more likely to have Cmin <1 mg/L (P = 0.02). There was a strong positive correlation between lopinavir and ritonavir concentrations. No associations were found between lopinavir AUC2-10 and age, sex, weight, nutritional status or mg/kg/dose of lopinavir.
Conclusions: These data do not support the use of 8-hourly lopinavir/ritonavir at studied doses. Evaluation of higher doses is needed to optimize treatment outcomes of TB and HIV in young children.
© The Author(s) 2019. Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- WHO. Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection: Recommendations for a Public Health Approach—Second Edition 2016; 97. http://www.who.int/hiv/pub/arv/arv-2016/en/. - PubMed
-
- McIlleron H, Ren Y, Nuttall J. et al. Lopinavir exposure is insufficient in children given double doses of lopinavir/ritonavir during rifampicin-based treatment for tuberculosis. Antivir Ther 2011; 16: 417–21. - PubMed
