

Zwitterionic poly-carboxybetaine coating reduces artificial lung thrombosis in sheep and rabbits
- PMID: 31082571
- PMCID: PMC6633914
- DOI: 10.1016/j.actbio.2019.05.019
Zwitterionic poly-carboxybetaine coating reduces artificial lung thrombosis in sheep and rabbits
Abstract
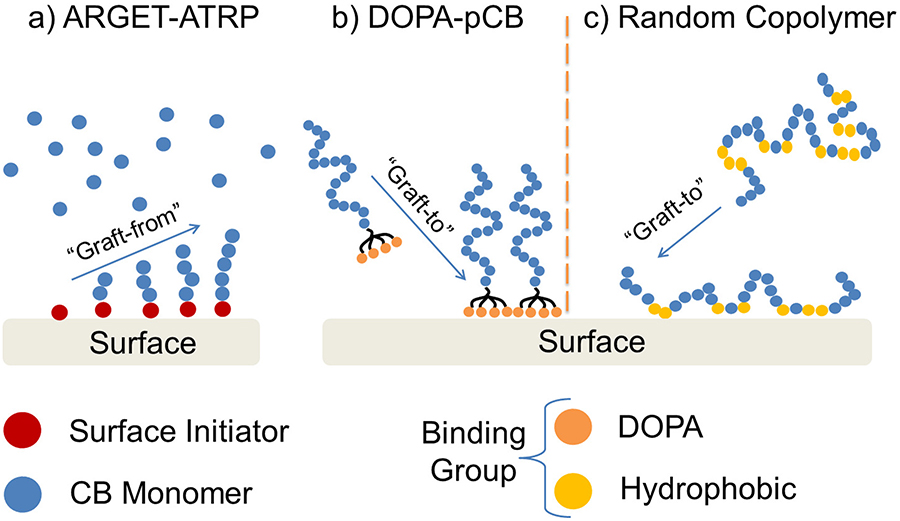
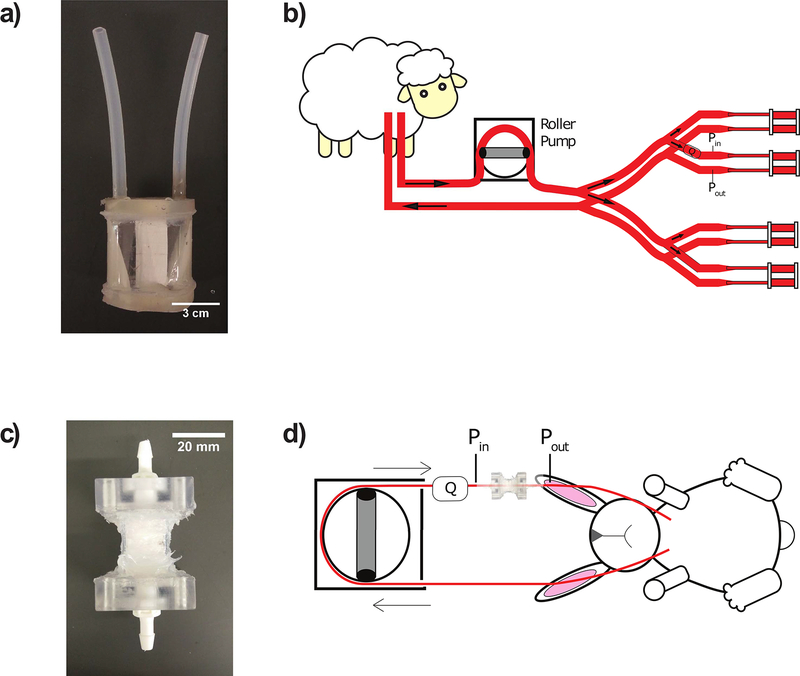
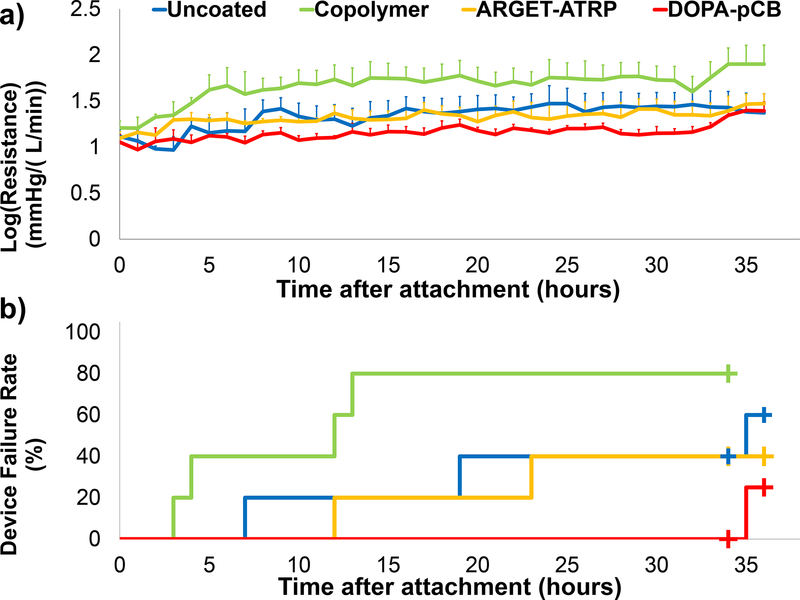
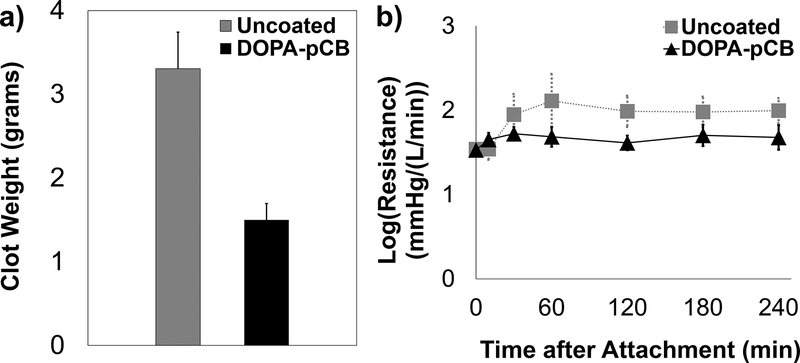
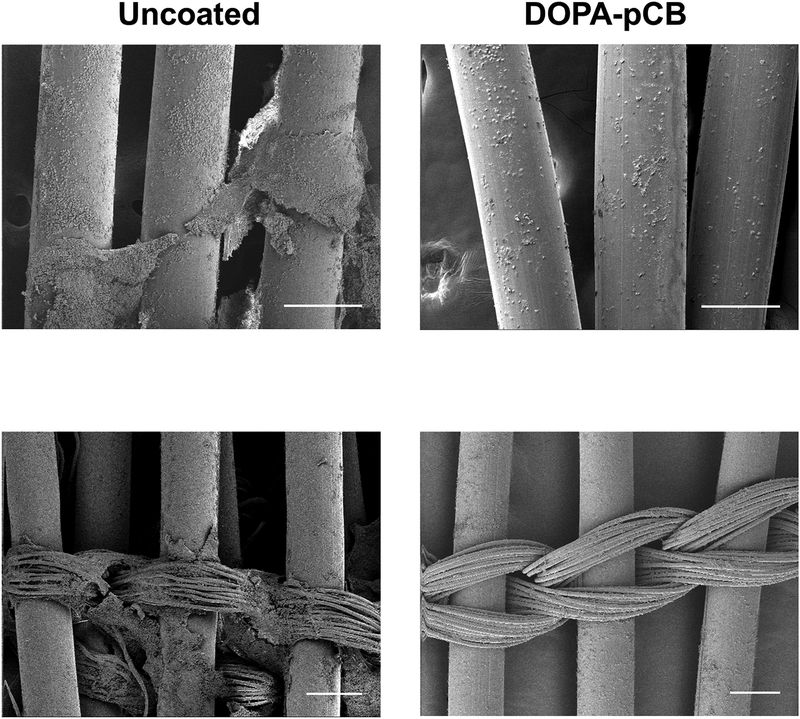
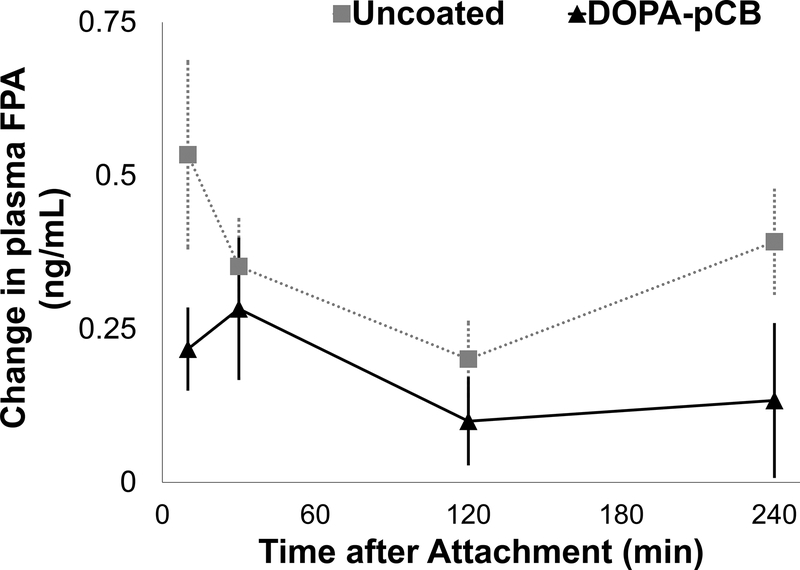
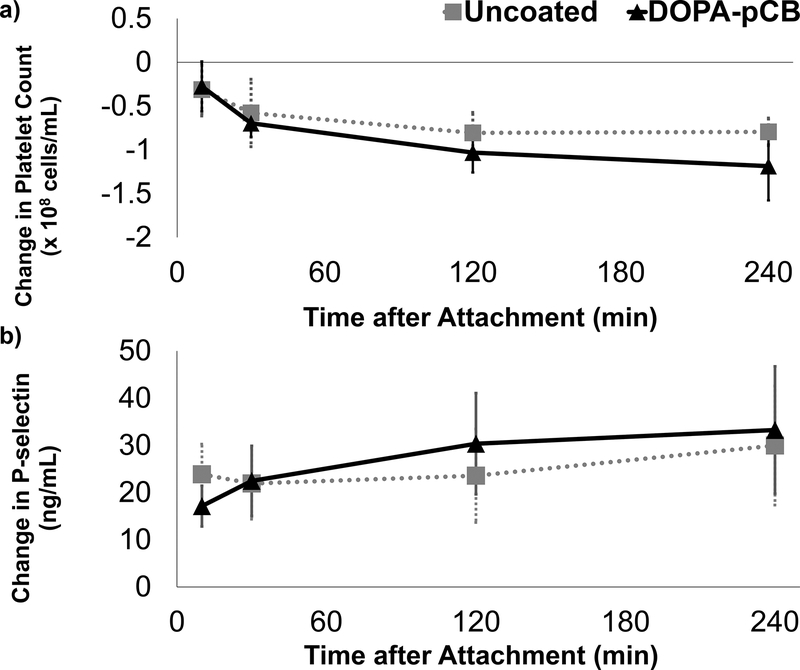
Current artificial lungs fail in 1-4 weeks due to surface-induced thrombosis. Biomaterial coatings may be applied to anticoagulate artificial surfaces, but none have shown marked long-term effectiveness. Poly-carboxybetaine (pCB) coatings have shown promising results in reducing protein and platelet-fouling in vitro. However, in vivo hemocompatibility remains to be investigated. Thus, three different pCB-grafting approaches to artificial lung surfaces were first investigated: 1) graft-to approach using 3,4-dihydroxyphenylalanine (DOPA) conjugated with pCB (DOPA-pCB); 2) graft-from approach using the Activators ReGenerated by Electron Transfer method of atom transfer radical polymerization (ARGET-ATRP); and 3) graft-to approach using pCB randomly copolymerized with hydrophobic moieties. One device coated with each of these methods and one uncoated device were attached in parallel within a veno-venous sheep extracorporeal circuit with no continuous anticoagulation (N = 5 circuits). The DOPA-pCB approach showed the least increase in blood flow resistance and the lowest incidence of device failure over 36-hours. Next, we further investigated the impact of tip-to-tip DOPA-pCB coating in a 4-hour rabbit study with veno-venous micro-artificial lung circuit at a higher activated clotting time of 220-300 s (N ≥ 5). Here, DOPA-pCB reduced fibrin formation (p = 0.06) and gross thrombus formation by 59% (p < 0.05). Therefore, DOPA-pCB is a promising material for improving the anticoagulation of artificial lungs. STATEMENT OF SIGNIFICANCE: Chronic lung diseases lead to 168,000 deaths each year in America, but only 2300 lung transplantations happen each year. Hollow fiber membrane oxygenators are clinically used as artificial lungs to provide respiratory support for patients, but their long-term viability is hindered by surface-induced clot formation that leads to premature device failure. Among different coatings investigated for blood-contacting applications, poly-carboxybetaine (pCB) coatings have shown remarkable reduction in protein adsorption in vitro. However, their efficacy in vivo remains unclear. This is the first work that investigates various pCB-coating methods on artificial lung surfaces and their biocompatibility in sheep and rabbit studies. This work highlights the promise of applying pCB coatings on artificial lungs to extend its durability and enable long-term respiratory support for lung disease patients.
Keywords: 3,4-Dihydroxyphenylalanine (DOPA); Artificial lung; Carboxybetaine; Thrombosis; Zwitterion.
Copyright © 2019 Acta Materialia Inc. Published by Elsevier Ltd. All rights reserved.
Figures
References
-
- Cystic Fibrosis Foundation Patient Registry 2016 Annual Data Report, Bethesda, Maryland, 2017.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
