

Defining and Predicting Early Recurrence in 957 Patients With Resected Pancreatic Ductal Adenocarcinoma
- PMID: 31082915
- PMCID: PMC6191366
- DOI: 10.1097/SLA.0000000000002734
Defining and Predicting Early Recurrence in 957 Patients With Resected Pancreatic Ductal Adenocarcinoma
Abstract
Objectives: To establish an evidence-based cut-off to differentiate between early and late recurrence and to compare clinicopathologic risk factors between the two groups.
Summary background data: A clear definition of "early recurrence" after pancreatic ductal adenocarcinoma resection is currently lacking.
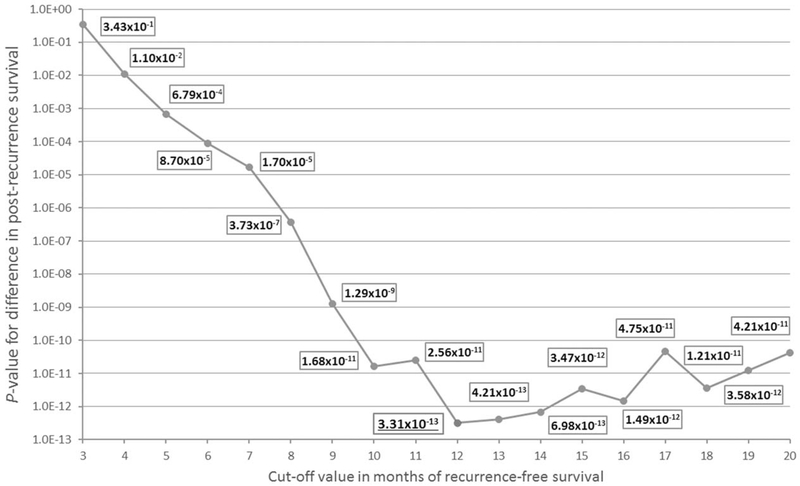
Methods: Patients undergoing pancreatectomy for pancreatic ductal adenocarcinoma between 2000 and 2013 were included. Exclusion criteria were neoadjuvant therapy and incomplete follow-up. A minimum P-value approach was used to evaluate the optimal cut-off value of recurrence-free survival to divide the patients into early and late recurrence cohorts based on subsequent prognosis. Potential risk factors for early recurrence were assessed with logistic regression models.
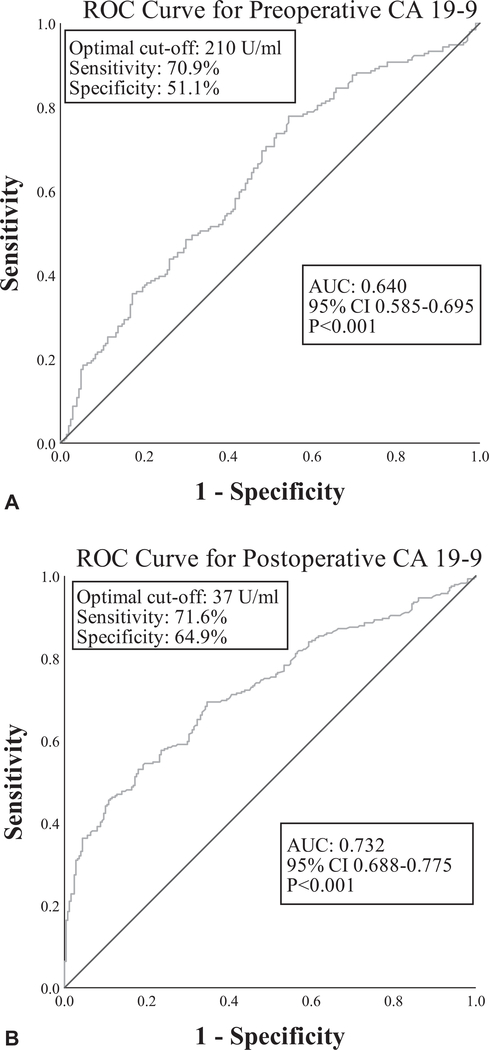
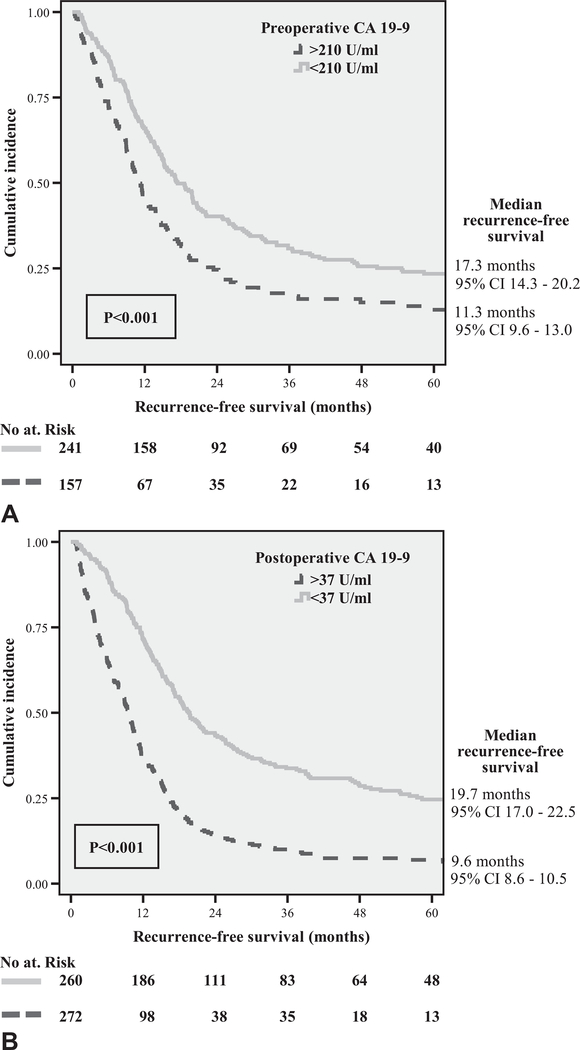
Results: Of 957 included patients, 204 (21.3%) were recurrence-free at last follow-up. The optimal length of recurrence-free survival to distinguish between early (n = 388, 51.5%) and late recurrence (n = 365, 48.5%) was 12 months (P < 0.001). Patients with early recurrence had 1-, and 2-year post-recurrence survival rates of 20 and 6% compared with 45 and 22% for the late recurrence group (both P < 0.001). Preoperative risk factors for early recurrence included a Charlson age-comorbidity index ≥4 (OR 1.65), tumor size > 3.0 cm on computed tomography (OR 1.53) and CA 19-9 > 210 U/mL (OR 2.30). Postoperative risk factors consisted of poor tumor differentiation grade (OR 1.66), microscopic lymphovascular invasion (OR 1.70), a lymph node ratio > 0.2 (OR 2.49), and CA 19-9 > 37 U/mL (OR 3.38). Adjuvant chemotherapy (OR 0.28) and chemoradiotherapy (OR 0.29) were associated with a reduced likelihood of early recurrence.
Conclusion: A recurrence-free interval of 12 months is the optimal threshold for differentiating between early and late recurrence, based on subsequent prognosis.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Rahib L, Smith BD, Aizenberg R, et al. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74:2913–2921. - PubMed
-
- Khorana AA, Mangu PB, Berlin J, et al. Potentially curable pancreatic cancer: american society of clinical oncology clinical practice guideline. J Clin Oncol. 2016;34:2541–2556. - PubMed
-
- Suenaga M, Fujii T, Kanda M, et al. Pattern of first recurrent lesions in pancreatic cancer: hepatic relapse is associated with dismal prognosis and portal vein invasion. Hepatogastroenterology. 2014;61:1756–1761. - PubMed
-
- Groot VP, Rezaee N, Wu W, et al. Patterns, timing, and predictors of recurrence following pancreatectomy for pancreatic ductal adenocarcinoma. Ann Surg. 2017. Epub ahead of Print. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
