

Associations Between Objective Sleep and Ambulatory Blood Pressure in a Community Sample
- PMID: 31083055
- PMCID: PMC6607429
- DOI: 10.1097/PSY.0000000000000711
Associations Between Objective Sleep and Ambulatory Blood Pressure in a Community Sample
Abstract
Objective: Epidemiologic data increasingly support sleep as a determinant of cardiovascular disease risk. Fewer studies have investigated the mechanisms underlying this relationship using objective sleep assessment approaches. Therefore, the aim of this study was to examine associations between daily blood pressure (BP) and both objectively assessed sleep duration and efficiency.
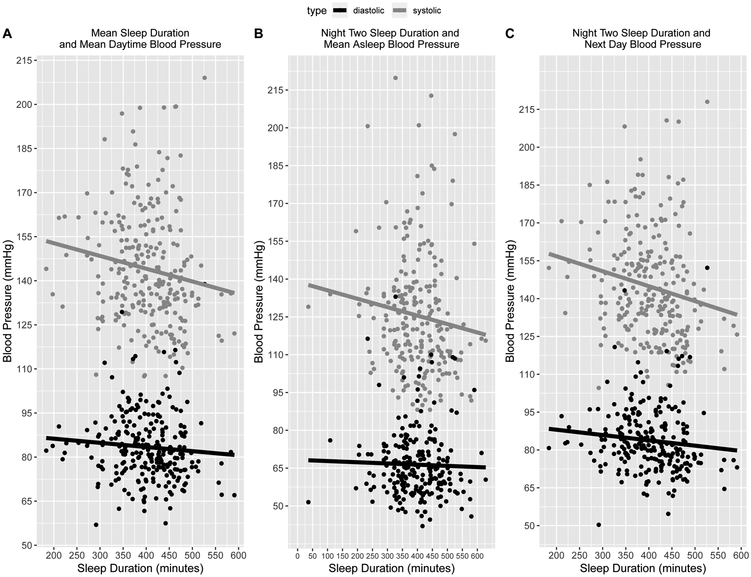
Methods: A diverse community sample of 300 men and women aged 21 to 70 years, enrolled in the North Texas Heart Study, participated in the study. Actigraphy-assessed sleep was monitored for two consecutive nights with ambulatory BP sampled randomly within 45-minute blocks on the first and second day as well as the second night.
Results: Overall, sleep duration results paralleled those of sleep efficiency. Individuals with lower sleep efficiency had higher daytime systolic (B = -0.35, SE = 0.11, p = .0018, R = 0.26) but not diastolic BP (B = -0.043, SE = 0.068, p = .52, R = 0.17) and higher nighttime BP (systolic: B = -0.37, SE = 0.10, p < .001, R = .15; diastolic: B = -0.20, SE = 0.059, p < .001, R = .14). Moreover, lower sleep efficiency on one night was associated with higher systolic (B = -0.51, SE = 0.11, p < .001, R = 0.23) and diastolic BP (B = -0.17, SE = 0.065, p = .012, R = .16) the following day. When 'asleep' BP was taken into account instead of nighttime BP, the associations between sleep and BP disappeared. When both sleep duration and efficiency were assessed together, sleep efficiency was associated with daytime systolic BP, whereas sleep duration was associated with nighttime BP.
Conclusions: Lower sleep duration and efficiency are associated with higher daytime systolic BP and higher nighttime BP when assessed separately. When assessed together, sleep duration and efficiency diverge in their associations with BP at different times of day. These results warrant further investigation of these possible pathways to disease.
Conflict of interest statement
Figures
References
-
- Badran M, Yassin BA, Fox N, Laher I, Ayas N. Epidemiology of Sleep Disturbances and Cardiovascular Consequences. Canadian Journal of Cardiology [Internet]. 2015. [cited 2017 July 26];31:873–79. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26037823 - PubMed
-
- Javaheri S, Redline S. Insomnia and Risk of Cardiovascular Disease. Chest [Internet]. 2017. [cited 2017 August 16];152:435–44. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28153671 - PMC - PubMed
-
- Wang X, Ouyang Y, Wang Z, Zhao G, Liu L, Bi Y. Obstructive sleep apnea and risk of cardiovascular disease and all-cause mortality: a meta-analysis of prospective cohort studies. International journal of cardiology [Internet]. 2013. [cited 2017 August 16];169:207–14. Available from: http://linkinghub.elsevier.com/retrieve/pii/S0167527313016719 - PubMed
-
- Li Y, Zhang X, Winkelman JW, Redline S, Hu FB, Stampfer M, Ma J, Gao X. Association between insomnia symptoms and mortality: a prospective study of U.S. men. Circulation [Internet]. 2014. [cited 2017 August 16];129:737–46. Available from: http://circ.ahajournals.org/cgi/doi/10.1161/CIRCULATIONAHA.113.004500 - DOI - PMC - PubMed
-
- Covassin N, Singh P. Sleep Duration and Cardiovascular Disease Risk. Sleep Medicine Clinics [Internet]. 2016. [cited 2016 December 7];11:81–89. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26972035 - PMC - PubMed
