

The re-emerging association between tuberculosis and diabetes: Lessons from past centuries
- PMID: 31085129
- PMCID: PMC6626679
- DOI: 10.1016/j.tube.2019.04.015
The re-emerging association between tuberculosis and diabetes: Lessons from past centuries
Abstract
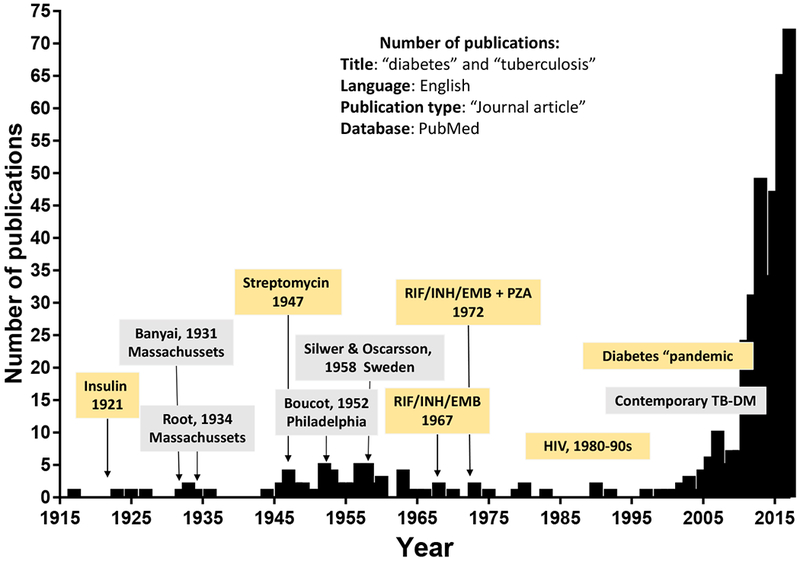
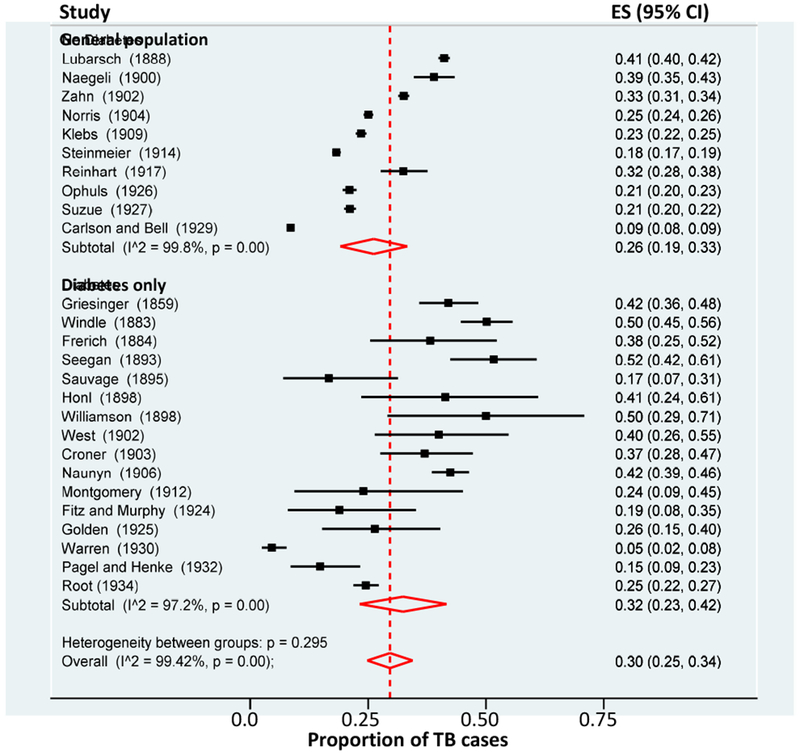
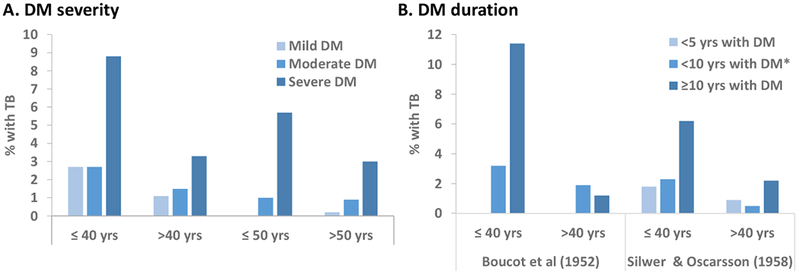
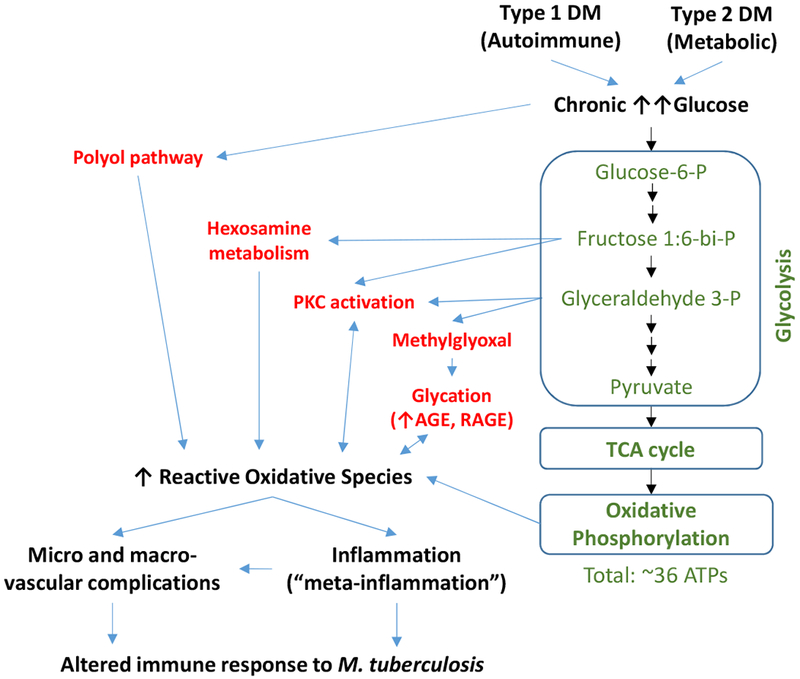
The association between tuberculosis (TB) and diabetes mellitus (DM) had a common place in the literature up to the first half of the 20th century, but virtually disappeared with the discovery of insulin to treat DM and antibiotics to cure TB. In the late 1990s the literature began to re-emerge with the worldwide increase in type 2 DM, particularly in TB-endemic countries. Today, type 2 DM is the most prevalent comorbidity among TB patients and the World Health Organization considers it a threat to TB control. We summarize the literature on TB and DM up to the 1960s. Then we evaluate unique aspects of this comorbidity in older times, such as the frequent diabetic comas that suggest challenges for proper DM management as insulin was being implemented, or the absence of antibiotics to cure TB. Despite the unique aspects of each study period, the literature across times is consistent in key aspects of the association. Namely, a higher TB prevalence among DM (versus non-DM patients), the importance of glucose control and chronic DM on TB susceptibility and the higher risk of death among patients with the co-morbidity. From the older literature, we can infer the likely contribution of type 1 DM to TB (in addition to type 2), regardless of their differing autoimmune or metabolic pathophysiology, respectively. Furthermore, in the older literature there was a notable reporting of DM development among TB patients, even though DM usually preceded TB. This observation deserves further epidemiological and basic studies to elucidate this intriguing aspect of the relationship between TB and DM.
Keywords: Death; History; Treatment outcomes; Tuberculosis; Type 1 diabetes; Type 2 diabetes.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Figures
References
-
- Riva MA. From milk to rifampicin and back again: history of failures and successes in the treatment for tuberculosis. J Antibiot (Tokyo). 2014;67(9):661–5. - PubMed
-
- American-Diabetes-Association. Standards of medical care in diabetes--2014. Diabetes Care. 2014;37 Suppl 1:S14–S80. - PubMed
-
- Ahlqvist E, Storm P, Karajamaki A, Martinell M, Dorkhan M, Carlsson A, et al. Novel subgroups of adult-onset diabetes and their association with outcomes: a data-driven cluster analysis of six variables. Lancet Diabetes Endocrinol. 2018;6(5):361–9. - PubMed
-
- Karamitsos DT. The story of insulin discovery. Diabetes Res Clin Pract. 2011;93 Suppl 1:S2–8. - PubMed
-
- Rosenfeld L Insulin: discovery and controversy. Clin Chem. 2002;48(12):2270–88. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
