

Internal hernias: a difficult diagnostic challenge. Review of CT signs and clinical findings
- PMID: 31085971
- PMCID: PMC6625567
- DOI: 10.23750/abm.v90i5-S.8344
Internal hernias: a difficult diagnostic challenge. Review of CT signs and clinical findings
Abstract
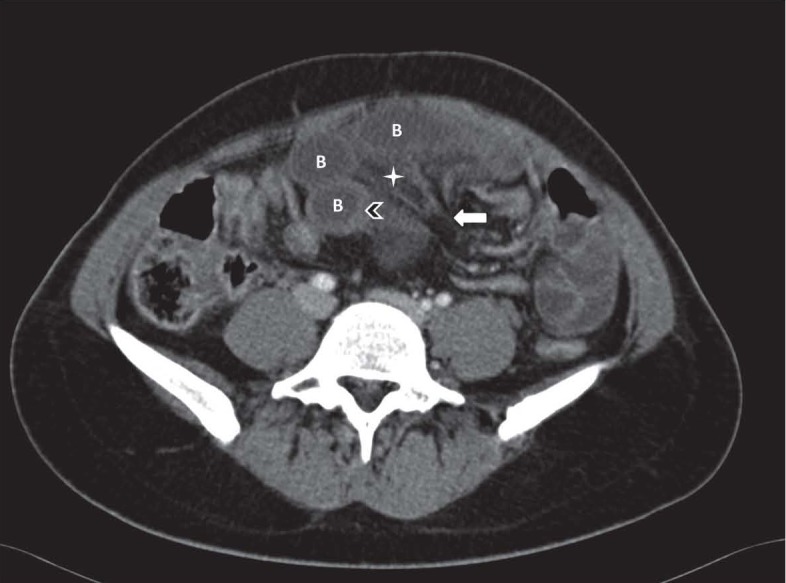
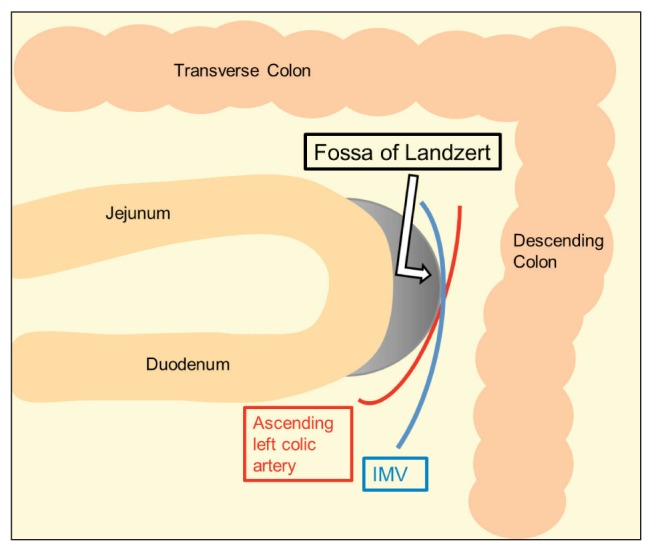
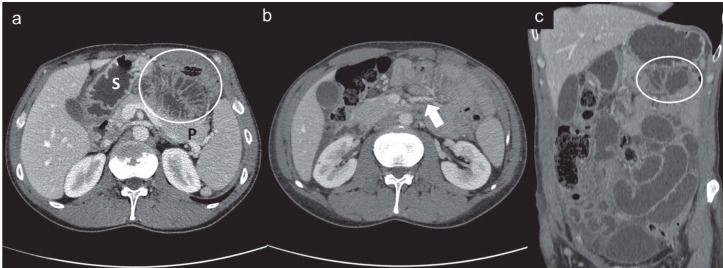
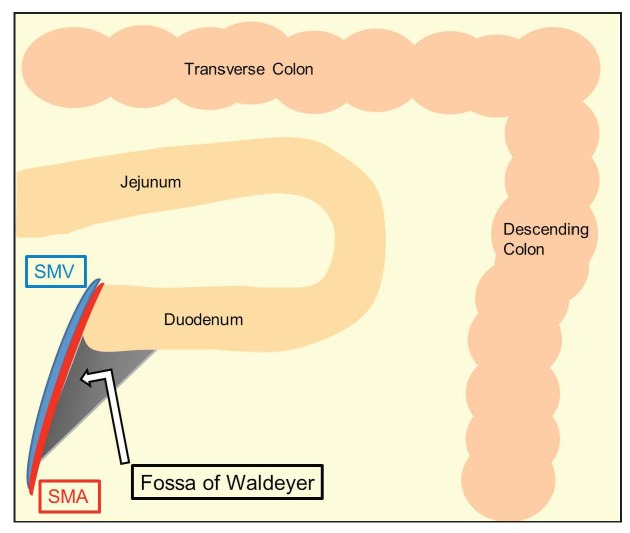
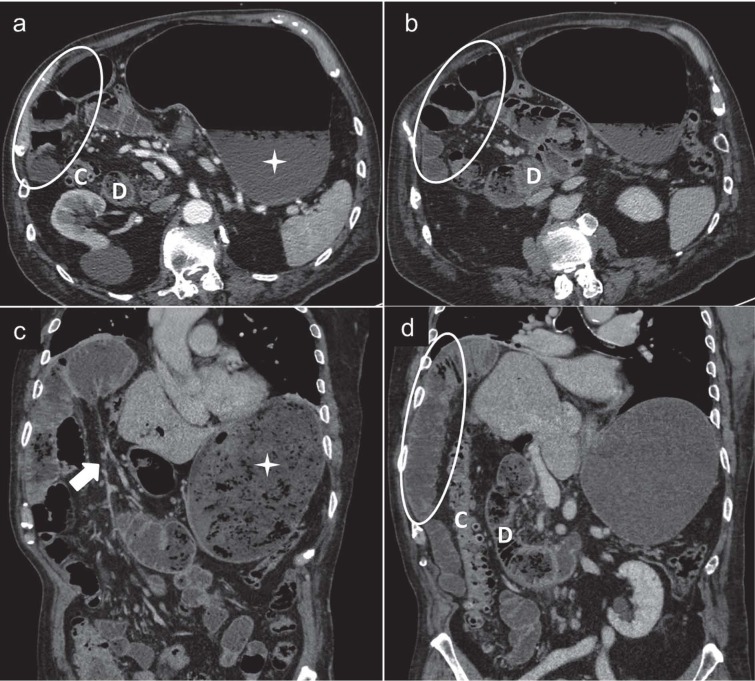
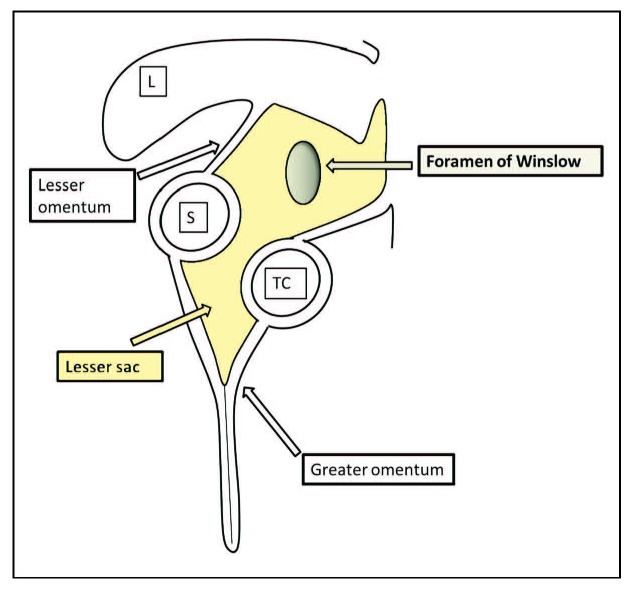
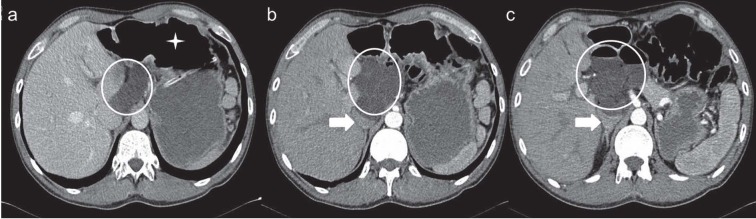
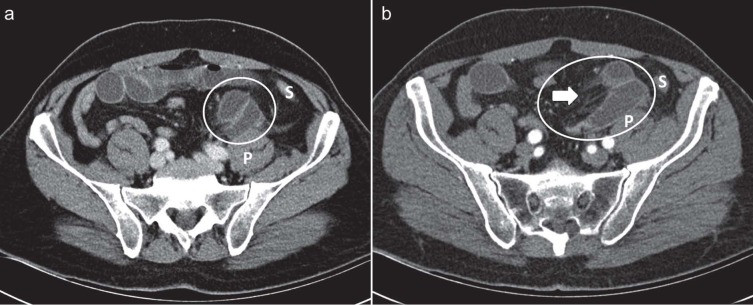
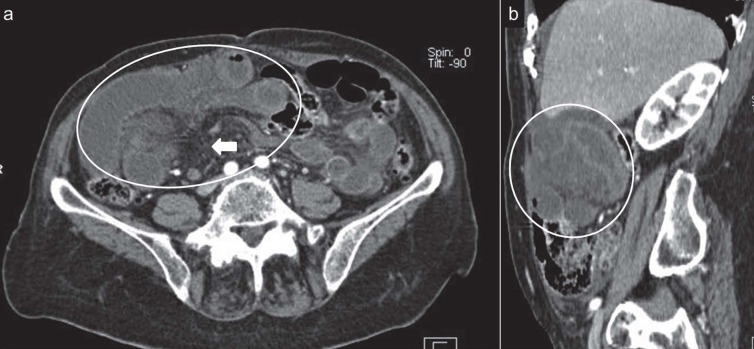
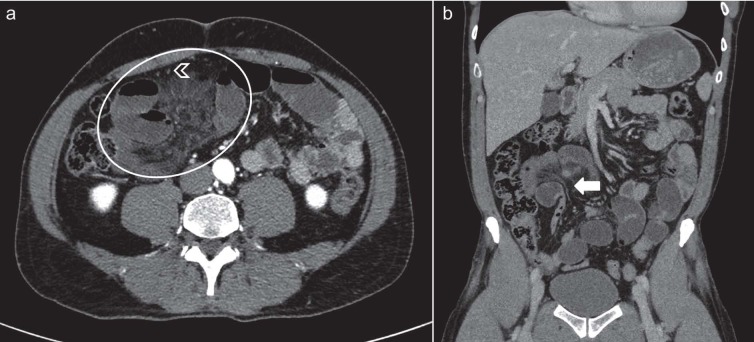
Although internal hernias are uncommon, they must be beared in mind in the differential diagnosis in cases of intestinal obstruction, especially in patients with no history of previous surgery or trauma. Because of the high possibility of strangulation and ischemia of the affected loops, internal hernias represent a potentially life-threatening condition and surgical emergency that needs to be quickly recognized and managed promptly. Imaging plays a leading role in the diagnosis and in particular multidetector computed tomography (MDCT), with its thin-section and high-resolution multiplanar reformatted (MPR) images, represents the first line image technique in these patients. The purpose of the present paper is to illustrate the characteristic anatomic location, the clinical findings and the CT appearance associated with main types of internal hernia, including paraduodenal, foramen of Winslow, pericecal, sigmoid-mesocolon- and trans-mesenteric- related, transomental, supravesical and pelvic hernias.
Figures




References
-
- Miller PA, Mezwa DG, Feczko PJ, Jafri ZH, Madrazo BL. Imaging of abdominal hernias. Radiographics. 1995;15:333–47. - PubMed
-
- Takeyama N, Gokan T, Ohgiya Y, et al. CT of internal hernias. Radiographics. 2005;25:997–1015. - PubMed
-
- Akyildiz H, Artis T, Sozuer E, et al. Internal hernia: complex diagnostic and therapeutic problem. Int J Surg. 2009;7:334–7. - PubMed
-
- Caranci F, Napoli M, Cirillo M, Briganti G, Brunese L, Briganti F. Basilar artery hypoplasia. Neuroradiol J. 2012;25:739–43. - PubMed
-
- Cirillo M, Caranci F, Tortora F, et al. Structural neuroimaging in dementia. J Alzheimers Dis. 2012;29:16–19.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
