

High intimal flap mobility assessed by intravascular ultrasound is associated with better short-term results after TEVAR in chronic aortic dissection
- PMID: 31086282
- PMCID: PMC6513991
- DOI: 10.1038/s41598-019-43856-6
High intimal flap mobility assessed by intravascular ultrasound is associated with better short-term results after TEVAR in chronic aortic dissection
Abstract
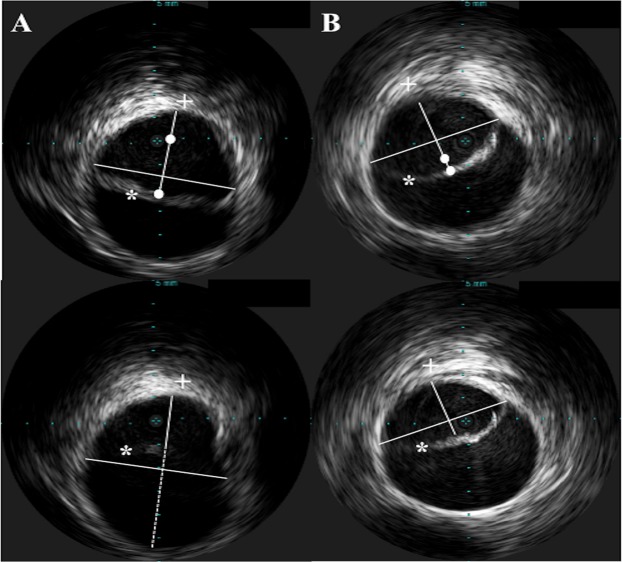
Thoracic endovascular aortic repair (TEVAR) in chronic aortic dissection remains controversial. We analysed whether a high intimal flap mobility (IFM) of the dissection membrane has an impact on aortic remodelling after TEVAR in chronic Type B aortic dissection. Patients undergoing TEVAR with intravascular ultrasound (IVUS) were analysed and IFM was calculated. High IFM was defined as maximum flap amplitude >3 mm. For determining aortic remodelling, the degree of true lumen (TL) expansion was analysed in the last available follow-up CT. Fifty-two patients (63.6 ± 15.4 years) with a mean follow-up of 26.6 ± 20.7 months were analysed. The mobile flap group (n = 29) showed higher absolute TL expansion at the distal stent-graft (5.9 ± 3.1 vs. 3.3 ± 5.4 mm; p = 0.036) and a higher increase in TL diameter (18 ± 10 vs. 9 ± 15%; p = 0.017) compared to the non-mobile group (n = 23). Basic TEVAR-related outcome characteristics were comparable, but the mobile intimal flap group showed a lower re-intervention rate (3 vs. 8pts.; p = 0.032) in chronic dissections. High IFM in chronic Type B aortic dissection is linked to improved aortic remodelling and is associated with a lower re-intervention rate over time. IVUS assessment of IFM in chronic Type B aortic dissection might be helpful in identifying patients with better remodelling after TEVAR.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Rohlffs F, et al. Chronic type B aortic dissection: indications and strategies for treatment. J Cardiovasc Surg (Torino). 2015;56:231–238. - PubMed
-
- Fleerakkers J, Schepens M. How should we manage type B aortic dissections? Gen Thorac Cardiovasc Surg. 2017;8:1–9. - PubMed
-
- Erbel R, et al. ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC) Eur Heart J. 2014;35:2873–2926. doi: 10.1093/eurheartj/ehu281. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
