

Automatized, Standardized, and Patient-Tailored Progressive Walking-Adaptability Training: A Proof-of-Concept Study
- PMID: 31087062
- PMCID: PMC6602157
- DOI: 10.1093/ptj/pzz013
Automatized, Standardized, and Patient-Tailored Progressive Walking-Adaptability Training: A Proof-of-Concept Study
Abstract
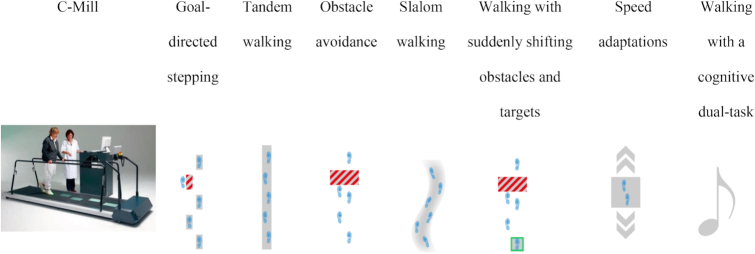
Background: Treadmill training augmented with visual images projected on the belt's surface can help improve walking adaptability. Moreover, patient-tailored automatization and standardization can increase the feasibility of walking-adaptability therapy. We developed C-Gait, a treadmill protocol consisting of a baseline walking-adaptability assessment involving 7 putatively distinct walking-adaptability tasks and a decision algorithm, to automatically update training content and execution parameters to a patients' performance and perceived challenge.
Objectives: The main objective was to examine the feasibility, acceptability, and clinical potential of C-Gait training. The secondary objective was to evaluate the validity of the baseline assessment.
Design: This was a longitudinal proof-of-concept study with pretraining, posttraining, and retention tests encompassing baseline assessment and walking-related clinical measures.
Methods: Twenty-four healthy adults, 12 healthy older persons, and 28 patients with gait and/or balance deficits performed the baseline assessment; the gait deficit group received 10 C-Gait training sessions over a 5-week period. Baseline assessment scores and walking-related clinical measures served as outcome measures.
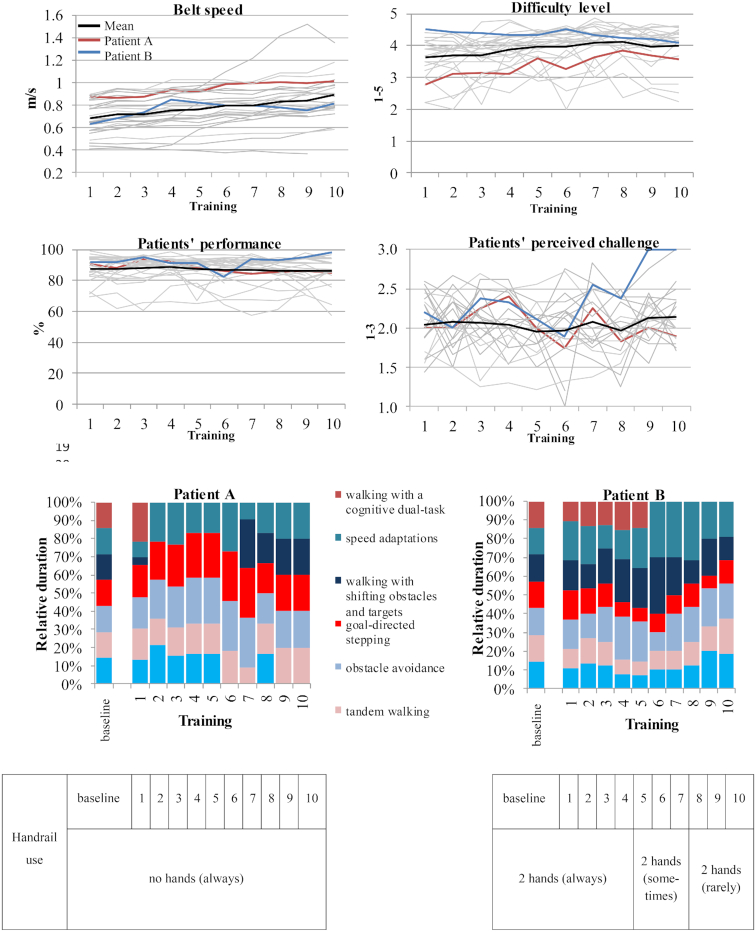
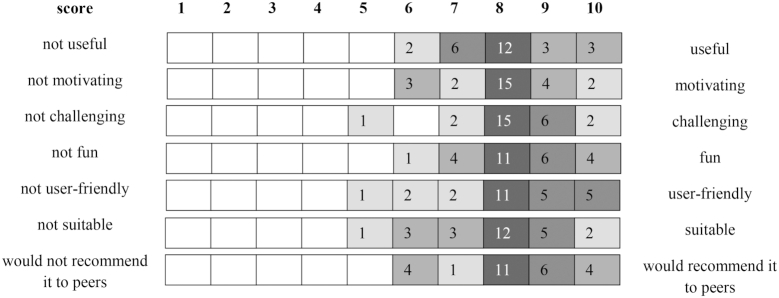
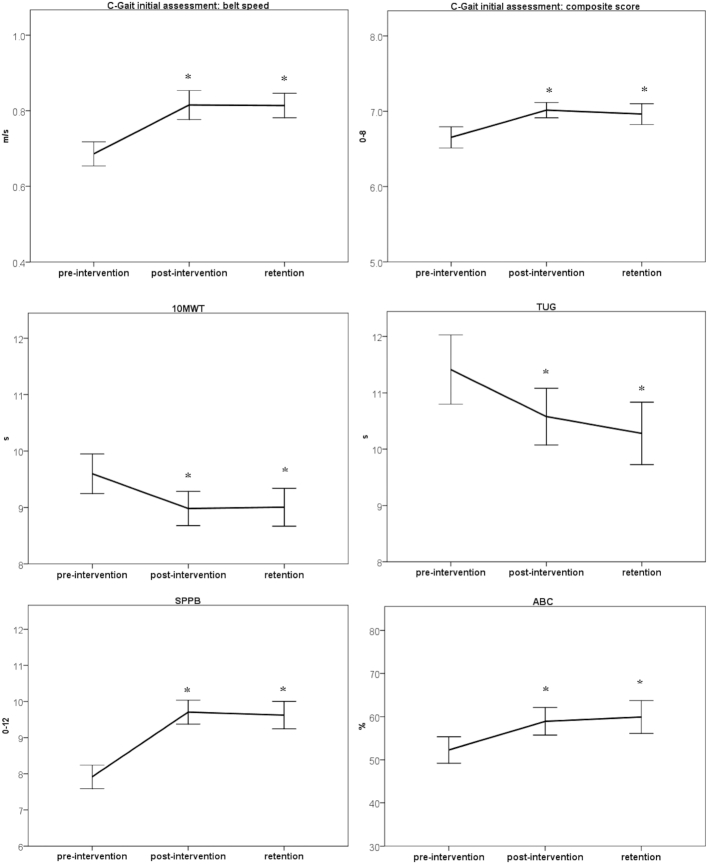
Results: C-Gait training exhibited significant progression in training content and execution, with considerable between-patient variation and minimal overruling by therapists. C-Gait training was well accepted and led to improvements in walking adaptability and general walking ability, which persisted after training cessation. Baseline assessment scores differed over groups and difficulty levels, had no-to-moderate correlations with walking-related clinical measures, and had limited correlations among walking-adaptability tasks.
Limitations: C-Gait was evaluated in a small yet diverse cohort. More encompassing studies are required to further establish its apparent merits. The validity of treadmill-based walking-adaptability assessment against an overground standard remains to be established.
Conclusions: C-Gait offers automatized, standardized, and patient-tailored walking-adaptability training that is feasible and well accepted, with good potential for improving task-specific and generic measures of walking.
© 2019 American Physical Therapy Association.
Figures
References
-
- Berg WP, Alessio HM, Mills MM, Tong C. Circumstances and consequences of falls in independent community-dwelling older adults. Age Ageing. 1997;26:261–268. - PubMed
-
- Tinetti ME, Speechley M, Ginter SF. Risk factors for falls among elderly persons living in the community. N Engl J Med. 1988;319:1701–1707. - PubMed
-
- Prudham D, Evans JG. Factors associated with falls in the elderly: a community study. Age Ageing. 1981;10:141–146. - PubMed
-
- Campbell AJ, Borrie MJ, Spears GF, Jackson SL, Brown JS, Fitzgerald JL. Circumstances and consequences of falls experienced by a community population 70 years and over during a prospective study. Age Ageing. 1990;19:136–141. - PubMed
-
- Said CM, Goldie PA, Patla AE, Sparrow WA, Martin KE. Obstacle crossing in subjects with stroke. Arch Phys Med Rehabil. 1999;80:1054–1059. - PubMed
