

Outcome of 881 total hip arthroplasties in 747 patients 21 years or younger: data from the Nordic Arthroplasty Register Association (NARA) 1995-2016
- PMID: 31088343
- PMCID: PMC6718182
- DOI: 10.1080/17453674.2019.1615263
Outcome of 881 total hip arthroplasties in 747 patients 21 years or younger: data from the Nordic Arthroplasty Register Association (NARA) 1995-2016
Abstract
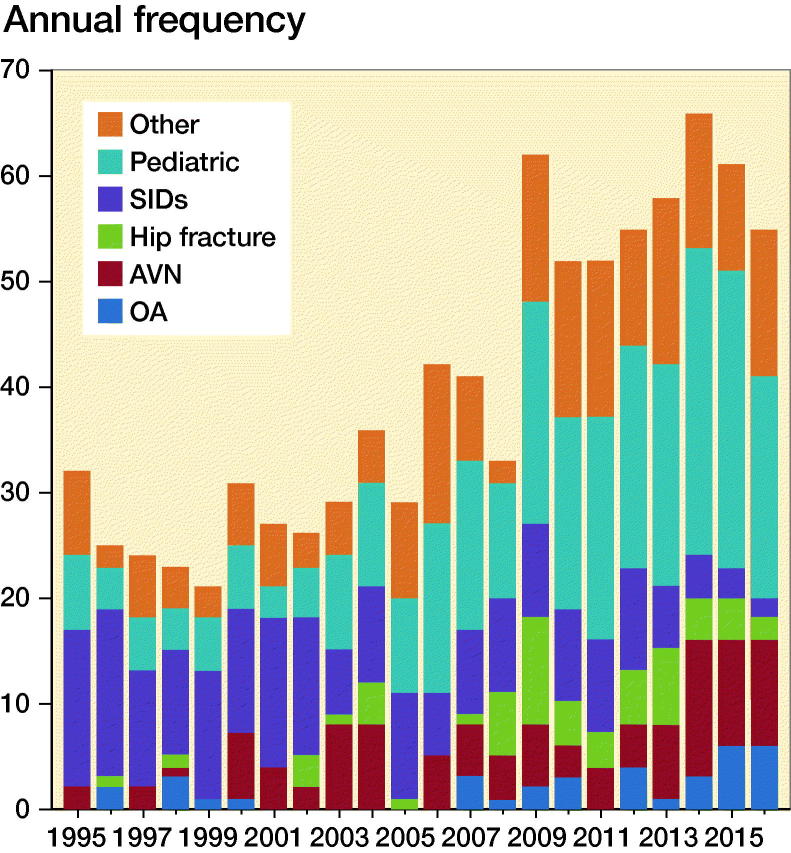
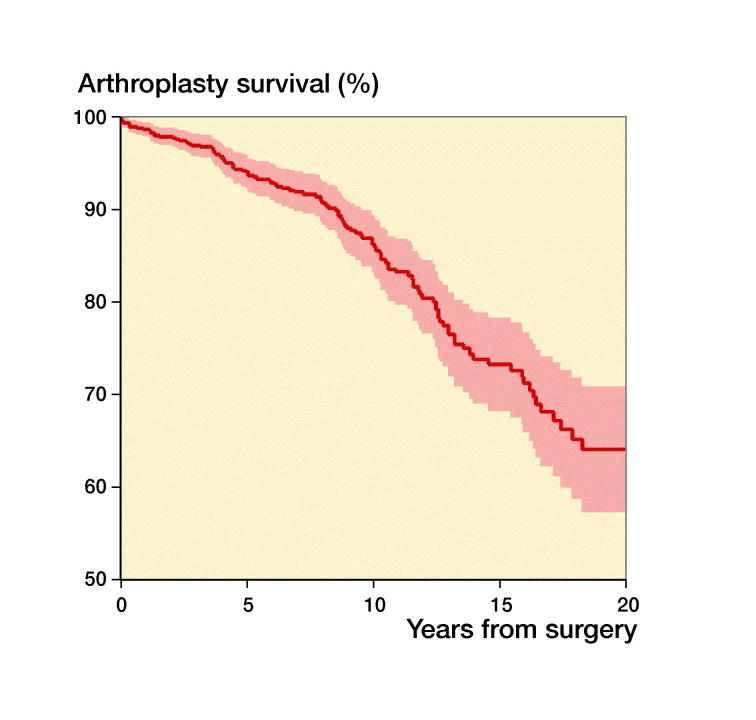
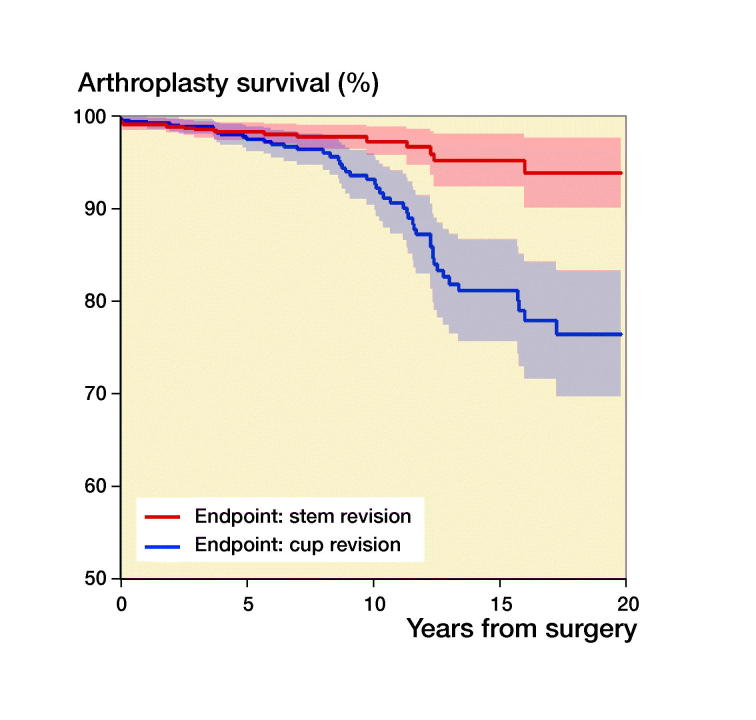
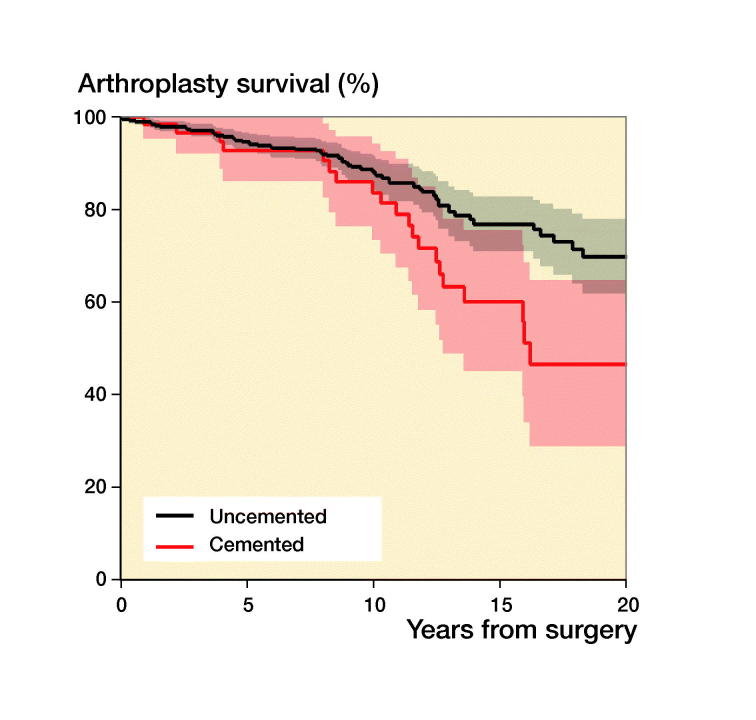
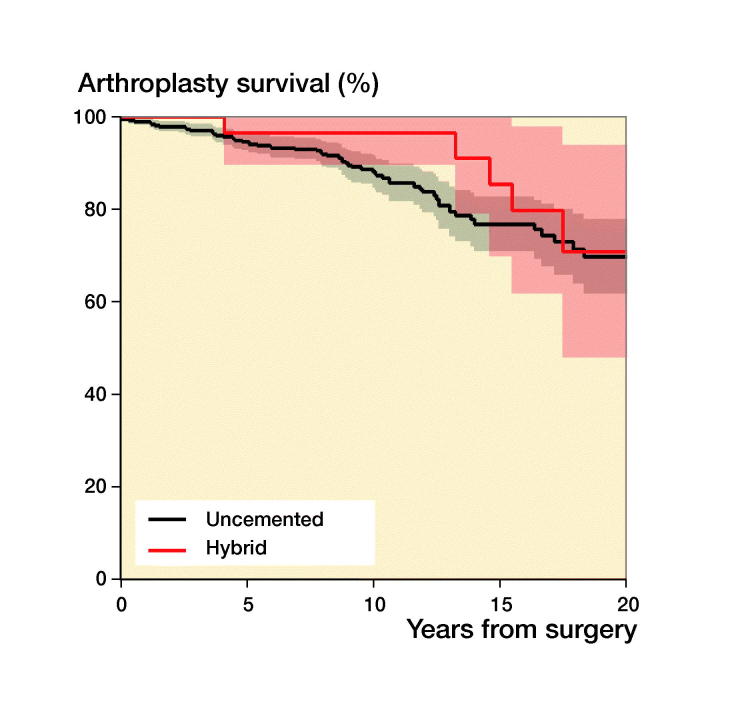
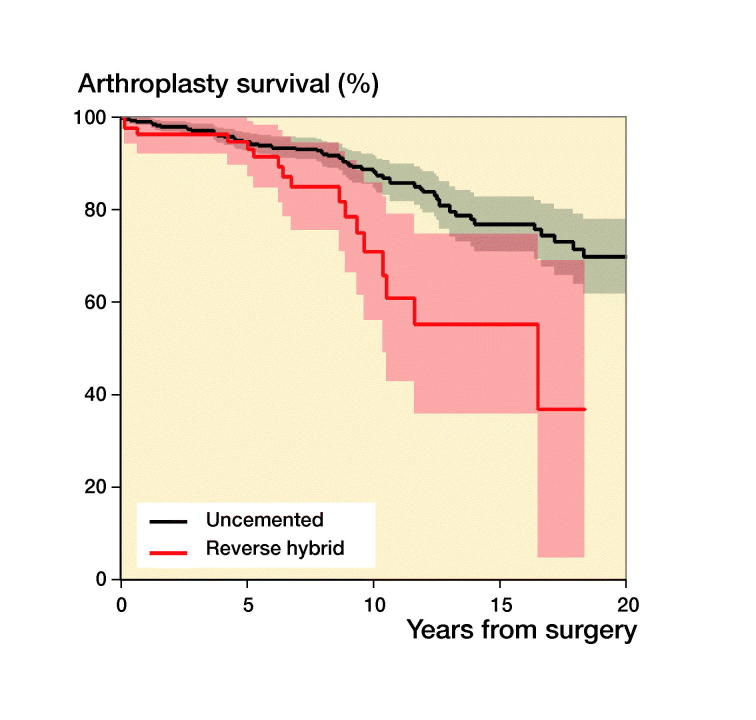
Background and purpose - The literature is scarce on the outcome of the youngest patients with total hip arthroplasties (THAs). We analyzed register data, revision risk, and related factors in patients 21 years or younger with THAs in the Nordic Arthroplasty Register Association (NARA). Patients and methods - We included all THA patients 21 years or younger reported during 1995 through 2016 to the Danish, Finnish, Norwegian, and Swedish hip arthroplasty registers and merged these into the NARA dataset. Primary outcome was any implant revision. Results - We identified 881 THAs in 747 patients. Mean age at primary surgery was 18 years (9-21). The indications for THA were pediatric hip diseases (33%), systemic inflammatory disease (23%), osteoarthritis (4%), avascular necrosis (12%), hip fracture sequelae (7%), and other diagnoses (21%). Unadjusted 10-year survival for all THAs was 86%. Comparison between indications showed no differences in survival. Uncemented implants were used most frequently. Survival for uncemented and cemented implants was the same adjusted for sex, indication, head size, and time period for primary surgery. Aseptic loosening was the main cause of revision. Interpretation - Both cemented and uncemented fixations seem to be a viable option in this age group, but with a lower implant survival than in older patient groups.
Figures
References
-
- Adelani M A, Mall N A, Nyazee H, Clohisy J C, Barrack R L, Nunley R M. Revision total hip arthroplasty with retained acetabular component. J Bone Joint Surg Am 2014; 96(12): 1015–20. - PubMed
-
- Berntson L, Andersson Gare B, Fasth A, Herlin T, Kristinsson J, Lahdenne P, Marhaug G, Nielsen S, Pelkonen P, Rygg M, Nordic Study G. Incidence of juvenile idiopathic arthritis in the Nordic countries: a population based study with special reference to the validity of the ILAR and EULAR criteria. J Rheumatol 2003; 30(10): 2275–82. - PubMed
-
- Cage D J, Granberry W M, Tullos H S. Long-term results of total arthroplasty in adolescents with debilitating polyarthropathy. Clin Orthop Relat Res 1992; (283): 156–62. - PubMed
-
- Chmell M J, Scott R D, Thomas W H, Sledge C B. Total hip arthroplasty with cement for juvenile rheumatoid arthritis: results at a minimum of ten years in patients less than thirty years old. J Bone Joint Surg Am 1997; 79(1): 44–52. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical