

Kidney autotransplantation for the treatment of renal artery occlusion after endovascular aortic repair: a case report
- PMID: 31088385
- PMCID: PMC6515634
- DOI: 10.1186/s12882-019-1353-7
Kidney autotransplantation for the treatment of renal artery occlusion after endovascular aortic repair: a case report
Abstract
Background: Unintentional renal artery occlusion after endovascular aneurysm repair (EVAR) for abdominal aortic aneurysm remains one of the most unfavorable complications. Renal salvage options include percutaneous transluminal renal artery angioplasty (PTRA) and open hepatosplenorenal bypass. However, the usefulness of kidney autotransplantation (AutoTx) remains unclear.
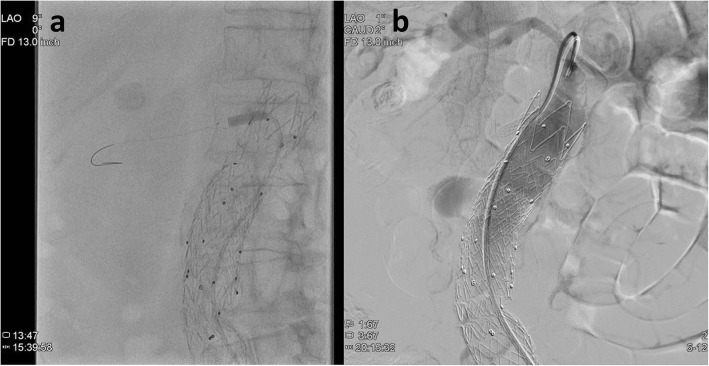
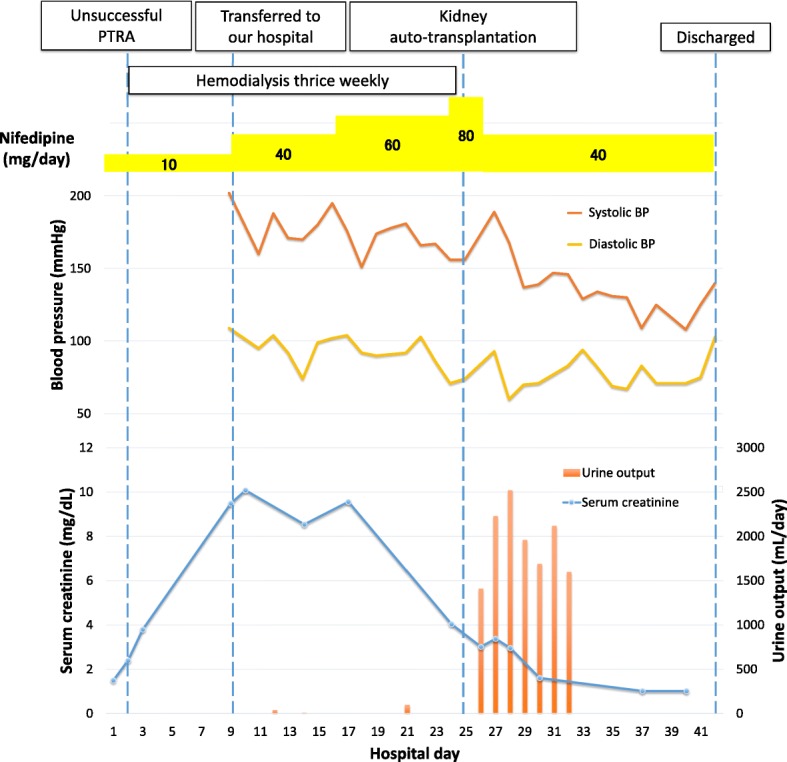
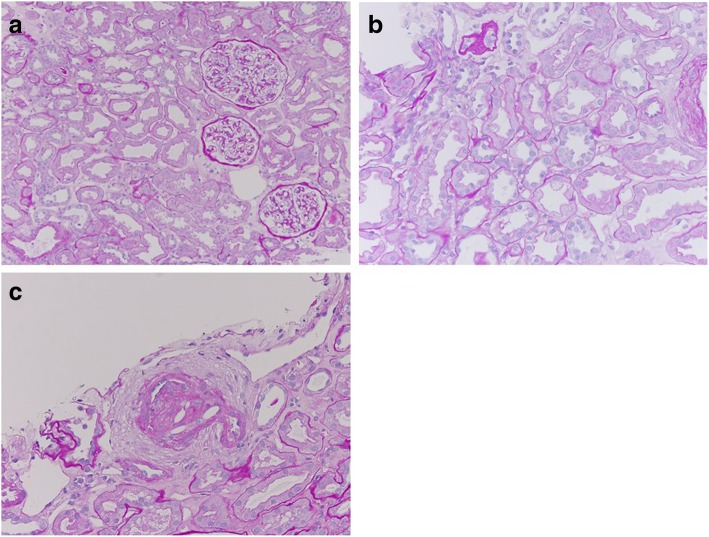
Case presentation: A 76-year-old woman with a right solitary kidney attributable to a left renal thromboembolism had previously undergone EVAR with a stent graft for an infrarenal aortic aneurysm, which led to ostial occlusion of the right renal artery. In addition, she had undergone PTRA and stenting. Two days before admission, she developed leg edema and hypertension, leading her to visit the hospital. Her serum creatinine level was 2.4 (baseline, 1.0) mg/dL. Acute kidney injury due to renal artery in-stent restenosis was suspected; re-angioplasty was attempted on day 2 of hospitalization, but was unsuccessful. Her renal function did not improve and anuria persisted; thus, hemodialysis was initiated on the same day. The right kidney size (8.6 cm) was preserved relative to her body size, with only mild cortical atrophy. Doppler ultrasonography and mercaptoacetyltriglycine scintigraphy revealed minimal but significant perfusion of the right kidney. Therefore, we considered that kidney perfusion was sustained and renal function could be reversed. On day 25 of hospitalization, right kidney AutoTx to the right iliac fossa was performed to reestablish adequate renal perfusion and reverse the need for dialysis. Soon after the procedure, the patient started passing urine. Her renal function improved; her serum creatinine level decreased to 1.0 mg/dL on day 33 of hospitalization. Hemodialysis was discontinued after the surgery. Zero-hour kidney biopsy showed only mild tubular injury, with neither tubular necrosis nor glomerular abnormalities.
Conclusions: Kidney AutoTx can be performed for patients with renal artery in-stent occlusion after unsuccessful PTRA who previously underwent EVAR. Our case showed successful recovery of renal function nearly 1 month after renal artery occlusion, indicating that revascularization should be considered even if it is delayed, as the kidney might be perfused through collateral circulation.
Keywords: Acute kidney injury; Collateral circulation; Endovascular aneurysm repair; Kidney autotransplantation; Percutaneous transluminal renal artery angioplasty; Renal artery occlusion.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this Case Report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Iwashima Y, Fukuda T, Yoshihara F, Kusunoki H, Kishida M, Hayashi S, et al. Incidence and risk factors for restenosis, and its impact on blood pressure control after percutaneous transluminal renal angioplasty in hypertensive patients with renal artery stenosis. J Hypertens. 2016;34:1407–1415. doi: 10.1097/HJH.0000000000000928. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
