

The impact of chlorhexidine bathing on hospital-acquired bloodstream infections: a systematic review and meta-analysis
- PMID: 31088521
- PMCID: PMC6518712
- DOI: 10.1186/s12879-019-4002-7
The impact of chlorhexidine bathing on hospital-acquired bloodstream infections: a systematic review and meta-analysis
Abstract
Background: Chlorhexidine gluconate (CHG) bathing of hospitalized patients may have benefit in reducing hospital-acquired bloodstream infections (HABSIs). However, the magnitude of effect, implementation fidelity, and patient-centered outcomes are unclear. In this meta-analysis, we examined the effect of CHG bathing on prevention of HABSIs and assessed fidelity to implementation of this behavioral intervention.
Methods: We undertook a meta-analysis by searching Medline, EMBASE, CINAHL, Scopus, and Cochrane's CENTRAL registry from database inception through January 4, 2019 without language restrictions. We included randomized controlled trials, cluster randomized trials and quasi-experimental studies that evaluated the effect of CHG bathing versus a non-CHG comparator for prevention of HABSIs in any adult healthcare setting. Studies of pediatric patients, of pre-surgical CHG use, or without a non-CHG comparison arm were excluded. Outcomes of this study were HABSIs, patient-centered outcomes, such as patient comfort during the bath, and implementation fidelity assessed through five elements: adherence, exposure or dose, quality of the delivery, participant responsiveness, and program differentiation. Three authors independently extracted data and assessed study quality; a random-effects model was used.
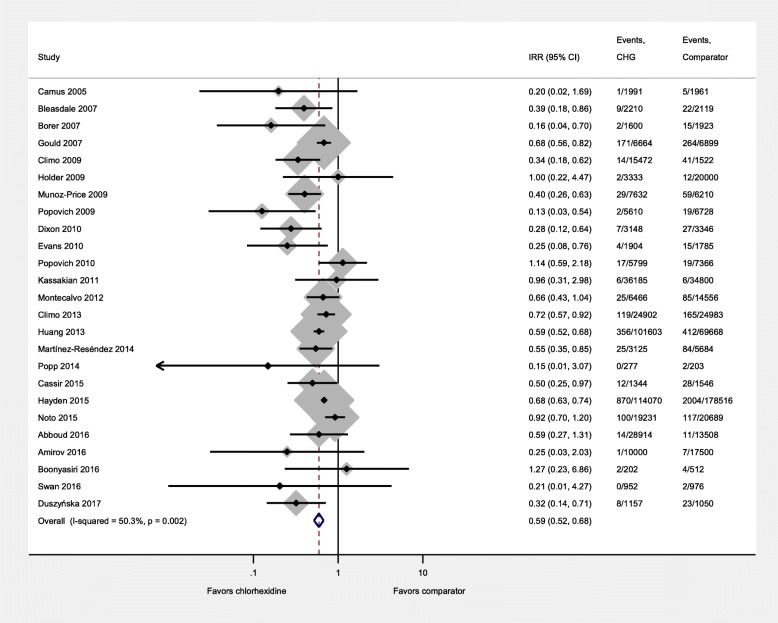
Results: We included 26 studies with 861,546 patient-days and 5259 HABSIs. CHG bathing markedly reduced the risk of HABSIs (IRR = 0.59, 95% confidence interval [CI]: 0.52-0.68). The effect of CHG bathing was consistent within subgroups: randomized (0.67, 95% CI: 0.53-0.85) vs. non-randomized studies (0.54, 95% CI: 0.44-0.65), bundled (0.66, 95% CI: 0.62-0.70) vs. non-bundled interventions (0.51, 95% CI: 0.39-0.68), CHG impregnated wipes (0.63, 95% CI: 0.55-0.73) vs. CHG solution (0.41, 95% CI: 0.26-0.64), and intensive care unit (ICU) (0.58, 95% CI: 0.49-0.68) vs. non-ICU settings (0.56, 95% CI: 0.38-0.83). Only three studies reported all five measures of fidelity, and ten studies did not report any patient-centered outcomes.
Conclusions: Patient bathing with CHG significantly reduced the incidence of HABSIs in both ICU and non-ICU settings. Many studies did not report fidelity to the intervention or patient-centered outcomes. For sustainability and replicability essential for effective implementation, fidelity assessment that goes beyond whether a patient received an intervention or not should be standard practice particularly for complex behavioral interventions such as CHG bathing.
Trial registration: Study registration with PROSPERO CRD42015032523 .
Keywords: Chlorhexidine bathing; Hospital-acquired bloodstream infections; Implementation; Infection prevention; Intervention fidelity; Patient-centered outcomes.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable (review of published literature).
Consent for publication
Not applicable.
Competing interests
Investigators will receive only normal scholarly gains from taking part in this study. The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Cassini A, Plachouras D, Eckmanns T, Abu Sin M, Blank HP, Ducomble T, et al. Burden of six healthcare-associated infections on European population health: estimating incidence-based disability-adjusted life years through a population prevalence-based modelling study. PLoS Med. 2016;13(10):e1002150. doi: 10.1371/journal.pmed.1002150. - DOI - PMC - PubMed
-
- DePalo VA, McNicoll L, Cornell M, Rocha JM, Adams L, Pronovost PJ. The Rhode Island ICU collaborative: a model for reducing central line-associated bloodstream infection and ventilator-associated pneumonia statewide. Qual Saf Health Care. 2010;19(6):555–561. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
