

Variation in Hospital-Based Rehabilitation Services Among Patients With Ischemic Stroke in the United States
- PMID: 31089705
- PMCID: PMC6489167
- DOI: 10.1093/ptj/pzz014
Variation in Hospital-Based Rehabilitation Services Among Patients With Ischemic Stroke in the United States
Abstract
Background: Little is known about variation in use of rehabilitation services provided in acute care hospitals for people who have had a stroke.
Objective: The objective was to examine patient and hospital sources of variation in acute care rehabilitation services provided for stroke.
Design: This was a retrospective, cohort design.
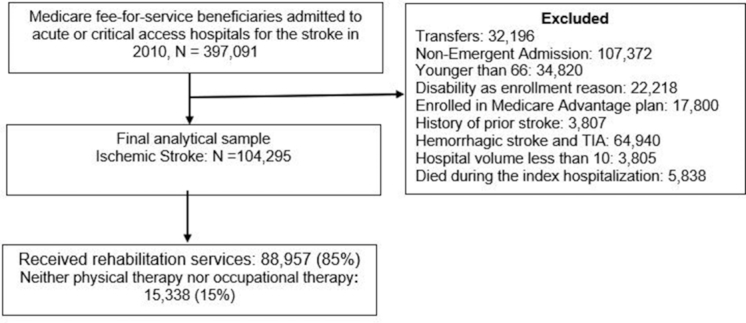
Methods: The sample consisted of Medicare fee-for-service beneficiaries with ischemic stroke admitted to acute care hospitals in 2010. Medicare claims data were linked to the Provider of Services file to gather information on hospital characteristics and the American Community Survey for sociodemographic data. Chi-square tests compared patient and hospital characteristics stratified by any rehabilitation use. We used multilevel, multivariable random effect models to identify patient and hospital characteristics associated with the likelihood of receiving any rehabilitation and with the amount of therapy received in minutes.
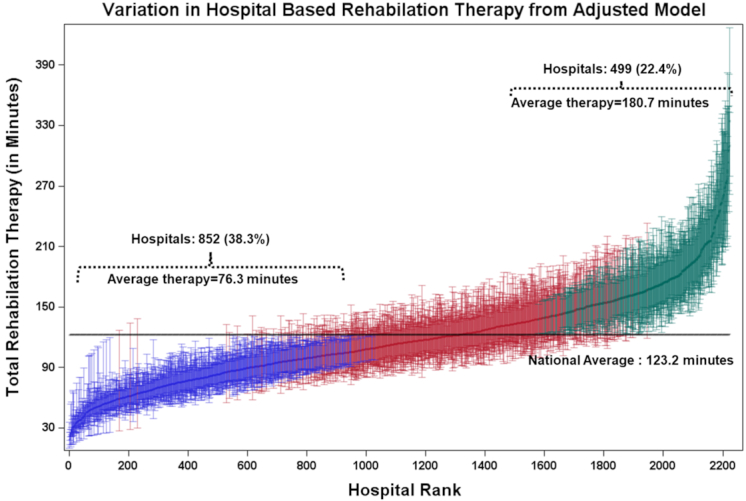
Results: Among 104,295 patients, 85.2% received rehabilitation (61.5% both physical therapy and occupational therapy; 22.0% physical therapy only; and 1.7% occupational therapy only). Patients received 123 therapy minutes on average (median [SD] = 90.0 [99.2] minutes) during an average length of stay of 4.8 [3.5] days. In multivariable analyses, male sex, dual enrollment in Medicare and Medicaid, prior hospitalization, ICU stay, and feeding tube were associated with lower odds of receiving any rehabilitation services. These same variables were generally associated with fewer minutes of therapy. Patients treated by tissue plasminogen activator, in limited-teaching and nonteaching hospitals, and in hospitals with inpatient rehabilitation units, were more likely to receive more therapy minutes.
Limitation: The findings are limited to patients with ischemic stroke.
Conclusion: Only 61% of patients with ischemic stroke received both physical therapy and occupational therapy services in the acute setting. We identified considerable variation in the use of rehabilitation services in the acute care setting following a stroke.
© 2019 American Physical Therapy Association.
Figures
References
-
- Craig LE, Bernhardt J, Langhorne P, Wu O. Early mobilization after stroke: an example of an individual patient data meta-analysis of a complex intervention. Stroke. 2010;41:2632–2636. - PubMed
-
- Cumming TB, Thrift AG, Collier JM et al.. Very early mobilization after stroke fast-tracks return to walking: further results from the phase II AVERT randomized controlled trial. Stroke. 2011;42:153–158. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
