

Cytokine removal in human septic shock: Where are we and where are we going?
- PMID: 31089920
- PMCID: PMC6517449
- DOI: 10.1186/s13613-019-0530-y
Cytokine removal in human septic shock: Where are we and where are we going?
Abstract
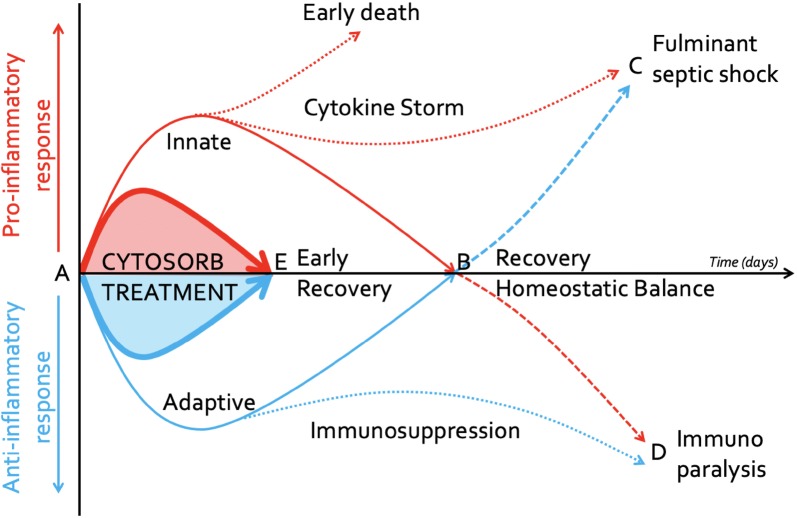
Although improving, the mortality from septic shock still remains high despite increased international awareness. As a consequence, much effort has focused on alternative treatment strategies in an effort to improve outcomes. The application of blood purification therapies to improve immune homeostasis has been suggested as one such method, but these approaches, such as high-volume continuous haemofiltration or cytokine and/or endotoxin removal, have enjoyed little success to date. More recently, the use of sorbent technologies has attracted much attention. These adsorbers are highly effective at removing inflammatory mediators, in particular, cytokines, from the bloodstream. This narrative review is the executive summary of meetings held throughout the 6th International Fluid Academy Days in Antwerp, Belgium (Nov 23-25, 2017), focusing on the current understanding regarding the use of such adsorbers in humans with septic shock. We followed a modified Delphi approach involving a combination of evidence appraisal together with expert opinion in order to achieve recommendations for practice and, importantly, future research.
Keywords: Blood purification; Cartridges; Cytokines; Cytosorb; DAMPS; Haemoperfusion; Immune modulation; PAMPS; Sepsis; Septic shock; Sorbents.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
Patrick M. Honore has served as consultant for Baxter, Gambro, Nikkiso and Asahi. He received honoraria for lectures from Baxter, Gambro, Nikkiso, Asahi, BBraun and Cytosorbents. Manu L.N.G. Malbrain is inaugural President of WSACS (The Abdominal Compartment Society,
Figures
References
-
- Machado FR, Cavalcanti AB, Bozza FA, SPREAD Investigators; Latin American Sepsis Institute Network et al. The epidemiology of sepsis in Brazilian intensive care units (the Sepsis PREvalence Assessment Database, SPREAD): an observational study. Lancet Infect Dis. 2017;17:1180–1189. doi: 10.1016/S1473-3099(17)30322-5. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
