

Ready-to-use therapeutic food (RUTF) for home-based nutritional rehabilitation of severe acute malnutrition in children from six months to five years of age
- PMID: 31090070
- PMCID: PMC6537457
- DOI: 10.1002/14651858.CD009000.pub3
Ready-to-use therapeutic food (RUTF) for home-based nutritional rehabilitation of severe acute malnutrition in children from six months to five years of age
Abstract
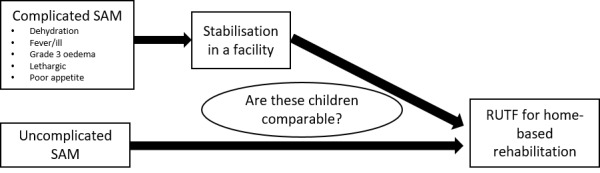
Background: Management of severe acute malnutrition (SAM) in children comprises two potential phases: stabilisation and rehabilitation. During the initial stabilisation phase, children receive treatment for dehydration, electrolyte imbalances, intercurrent infections and other complications. In the rehabilitation phase (applicable to children presenting with uncomplicated SAM or those with complicated SAM after complications have been resolved), catch-up growth is the main focus and the recommended energy and protein requirements are much higher. In-hospital rehabilitation of children with SAM is not always desirable or practical - especially in rural settings - and home-based care can offer a better solution. Ready-to-use therapeutic food (RUTF) is a widely used option for home-based rehabilitation, but the findings of our previous review were inconclusive.
Objectives: To assess the effects of home-based RUTF used during the rehabilitation phase of SAM in children aged between six months and five years on recovery, relapse, mortality and rate of weight gain.
Search methods: We searched the following databases in October 2018: CENTRAL, MEDLINE, Embase, six other databases and three trials registers. We ran separate searches for cost-effectiveness studies, contacted researchers and healthcare professionals in the field, and checked bibliographies of included studies and relevant reviews.
Selection criteria: Randomised controlled trials (RCTs) and quasi-RCTs, where children aged between six months and five years with SAM were, during the rehabilitation phase, treated at home with RUTF compared to an alternative dietary approach, or with different regimens and formulations of RUTF compared to each other. We assessed recovery, deterioration or relapse and mortality as primary outcomes; and rate of weight gain, time to recovery, anthropometrical changes, cognitive development and function, adverse outcomes and acceptability as secondary outcomes.
Data collection and analysis: We screened for eligible studies, extracted data and assessed risk of bias of those included, independently and in duplicate. Where data allowed, we performed a random-effects meta-analysis using Review Manager 5, and investigated substantial heterogeneity through subgroup and sensitivity analyses. For the main outcomes, we evaluated the quality of the evidence using GRADE, and presented results in a 'Summary of findings' table per comparison.
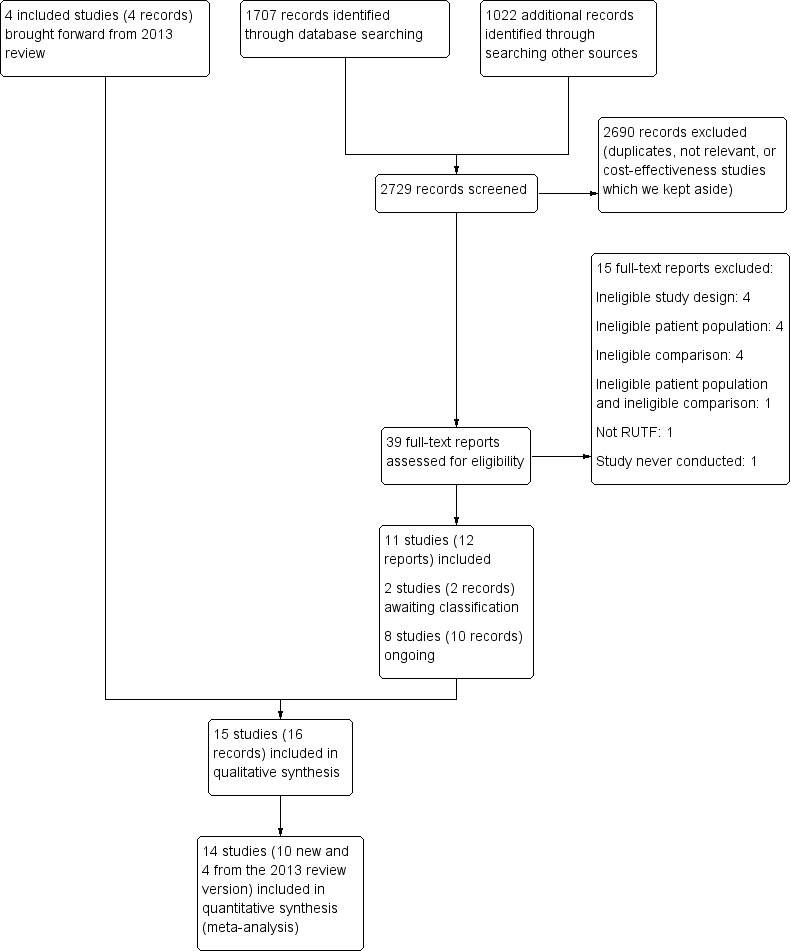
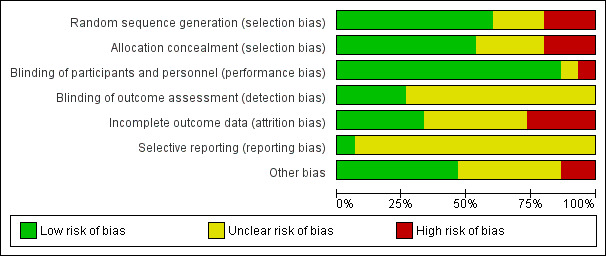
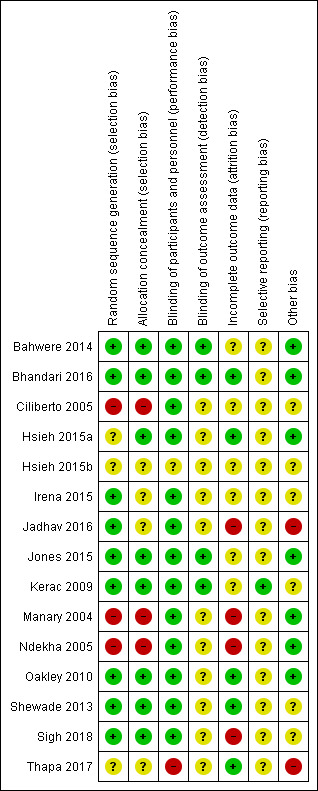
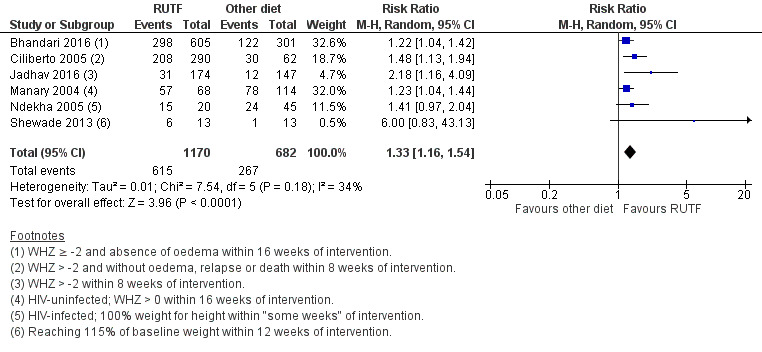
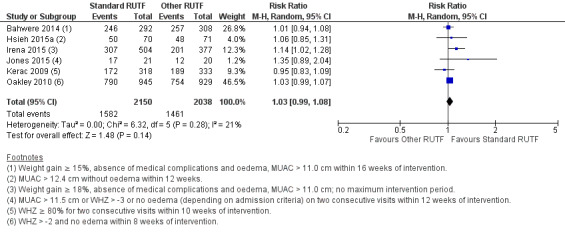
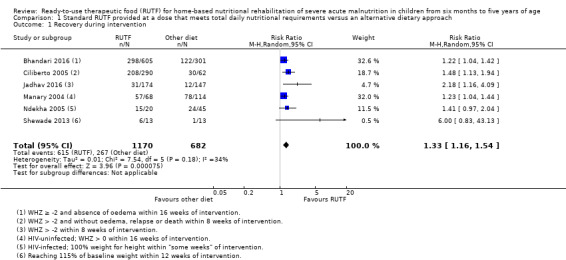
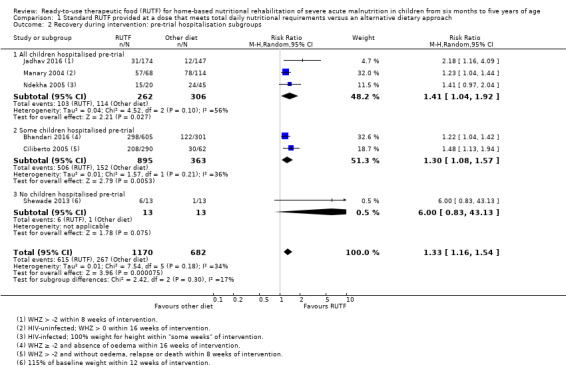
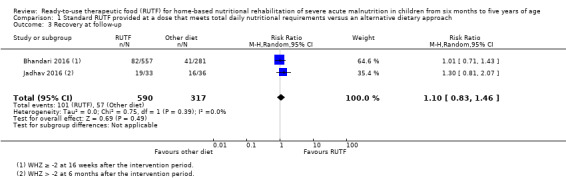
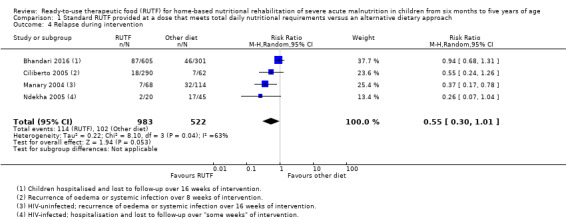
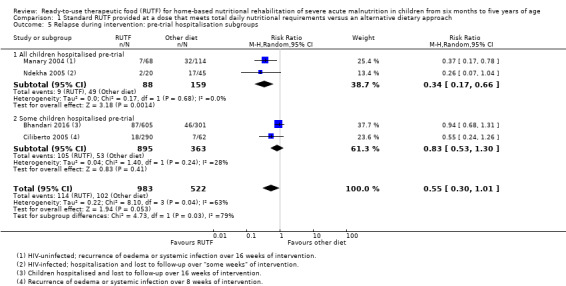
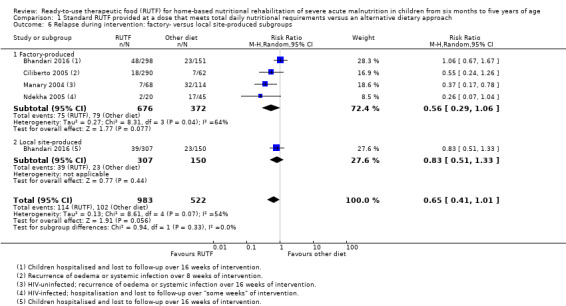
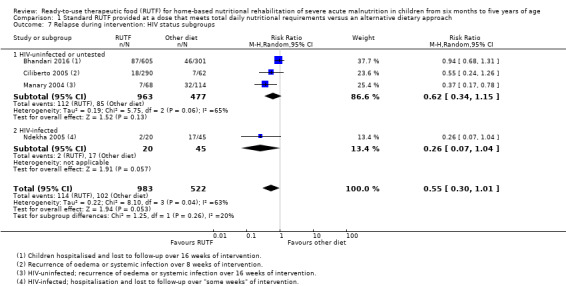
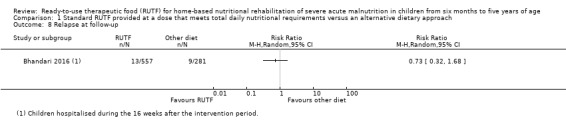
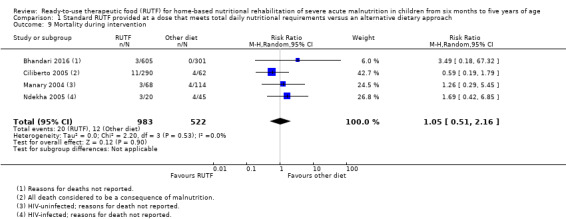
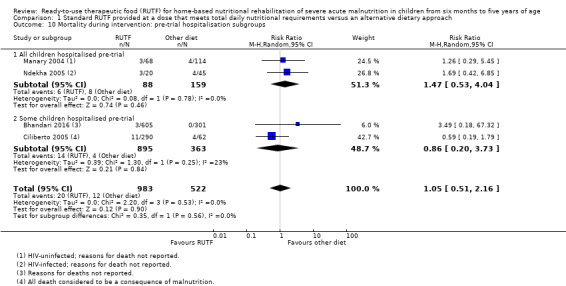
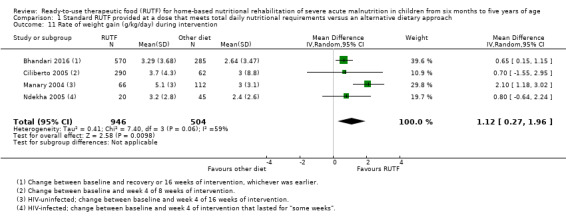
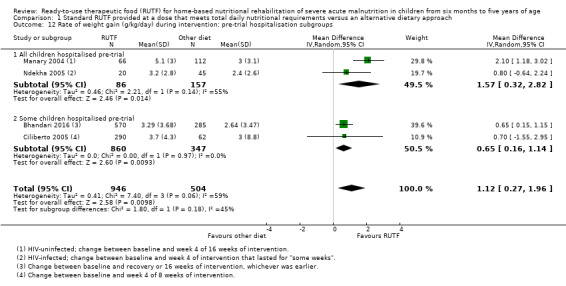
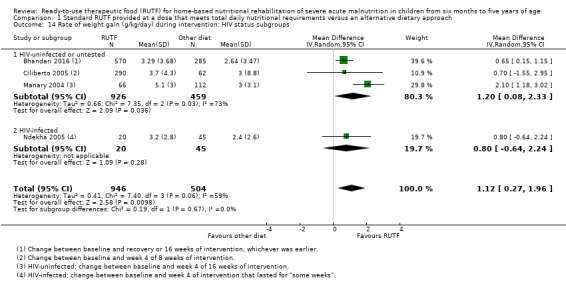
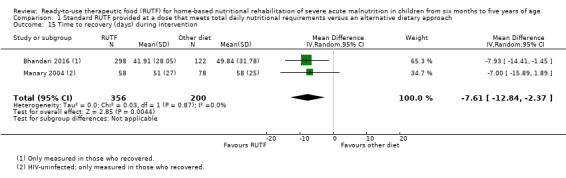
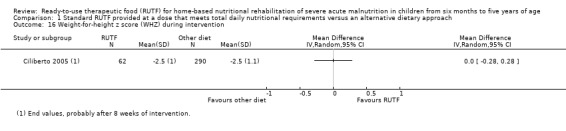
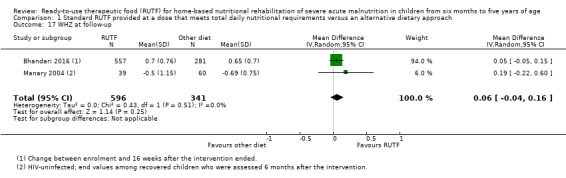
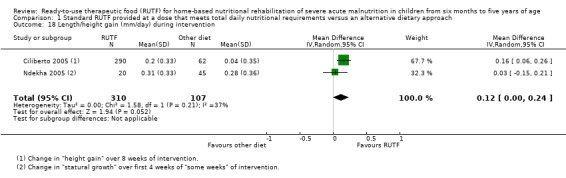
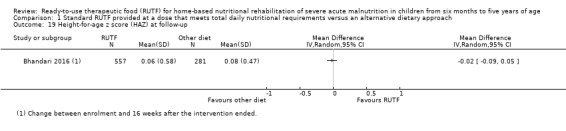
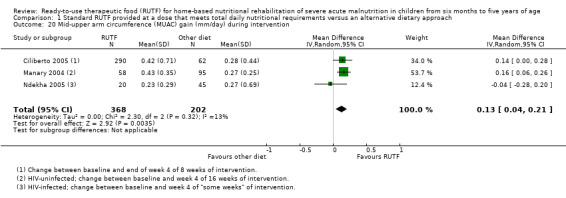
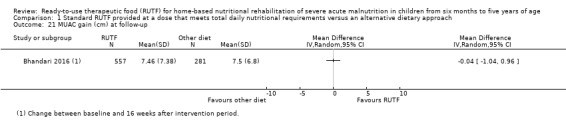
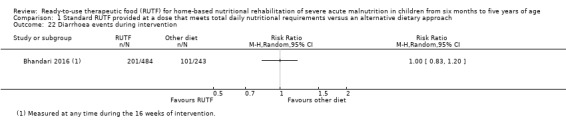
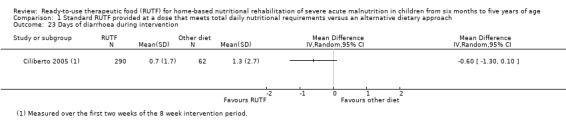
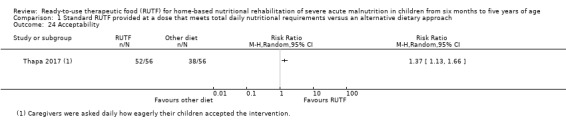
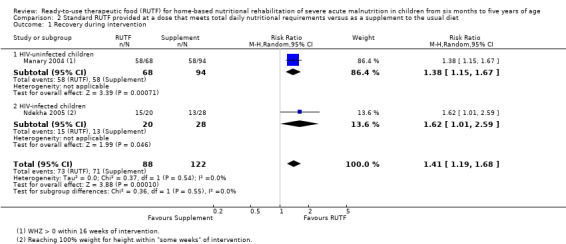
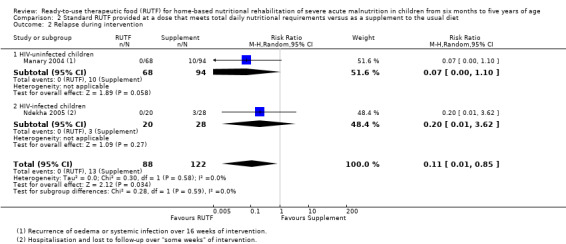
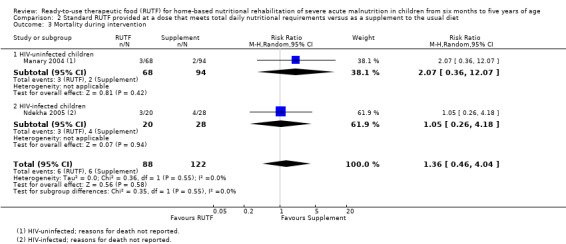
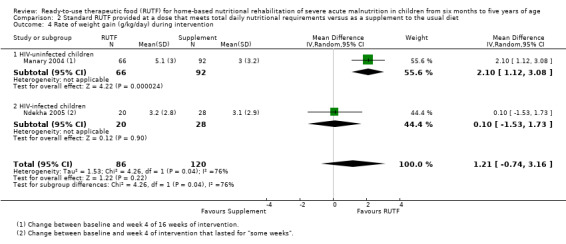
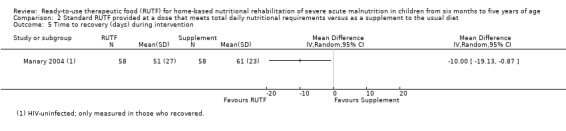
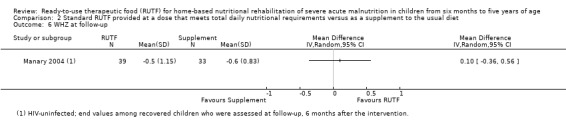
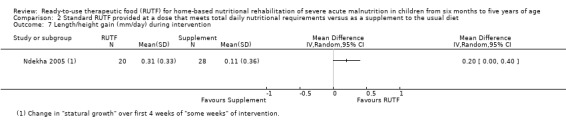
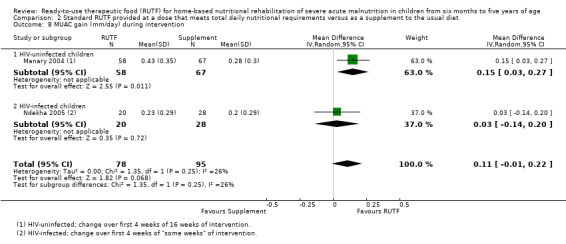
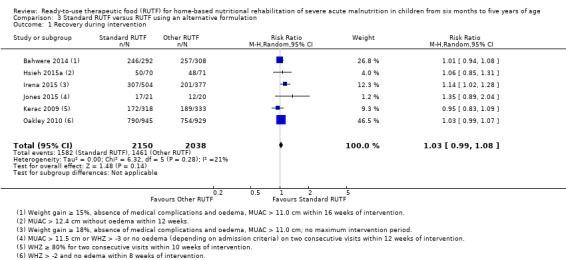
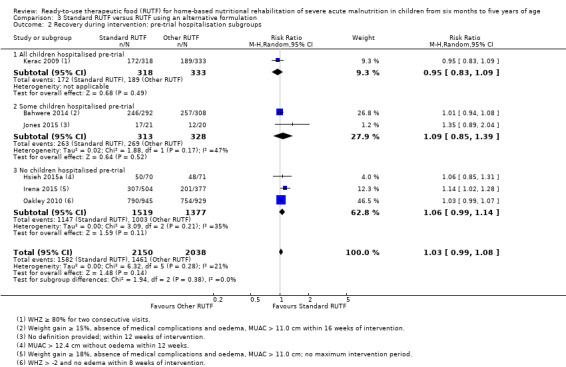
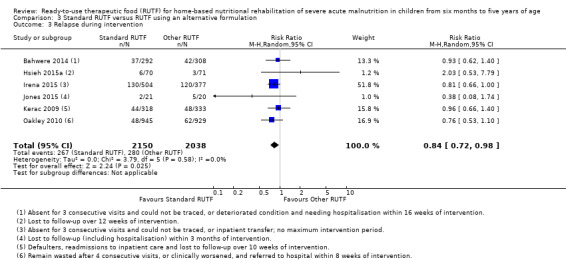
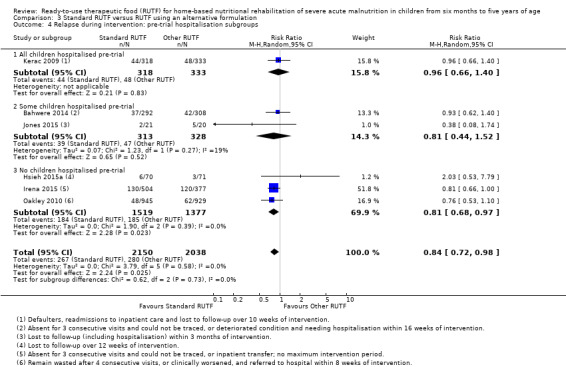
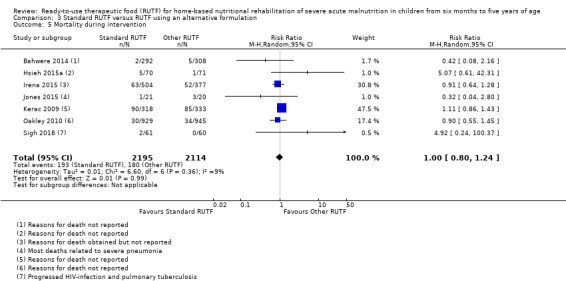
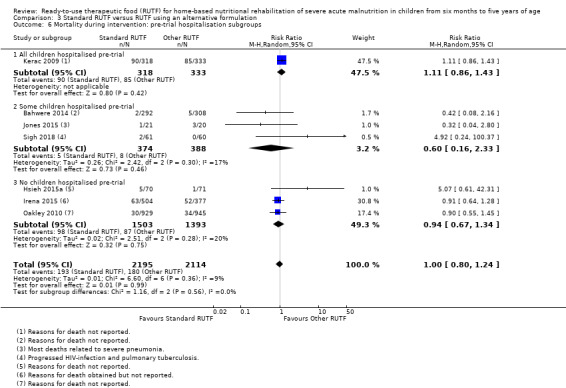
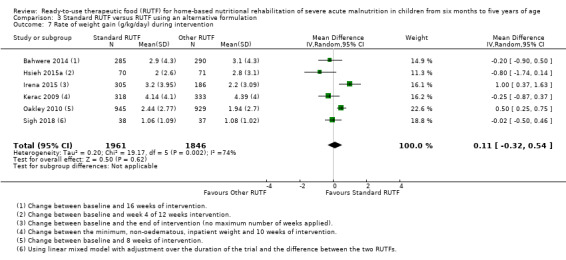
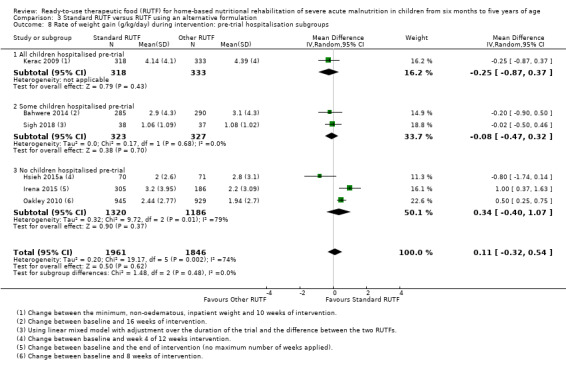
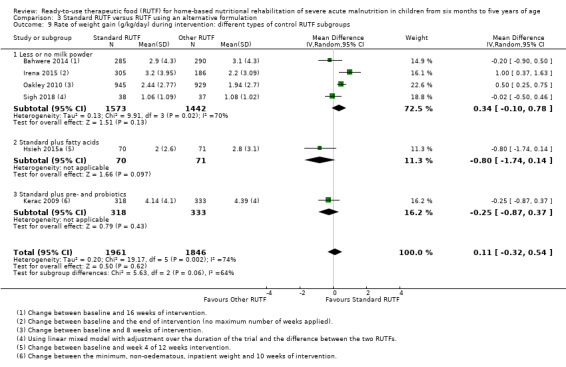
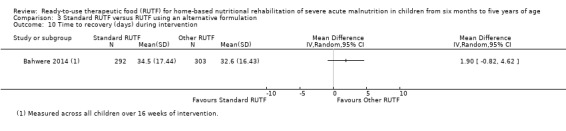
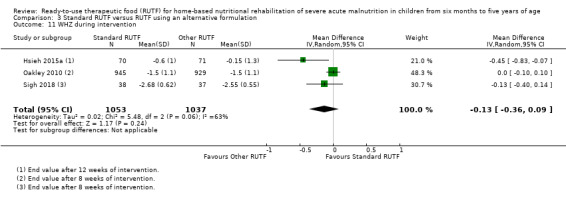
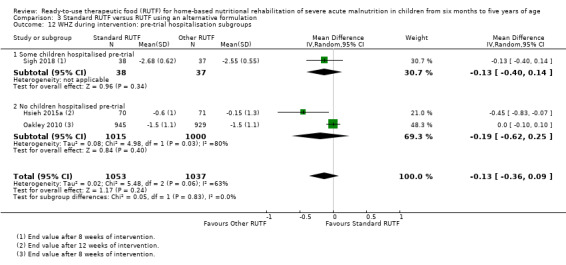
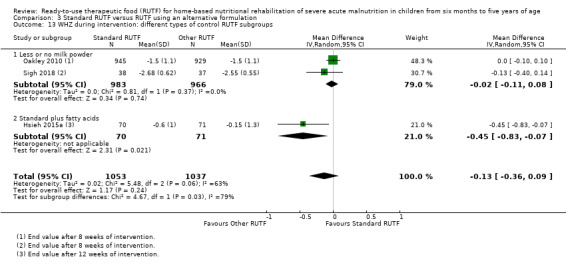
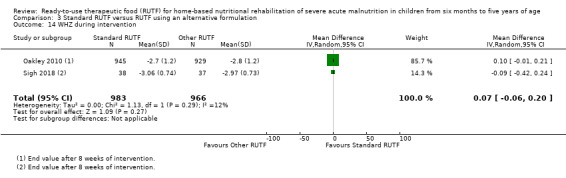
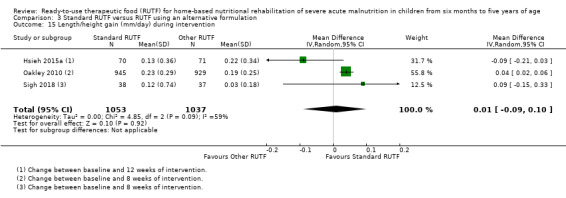
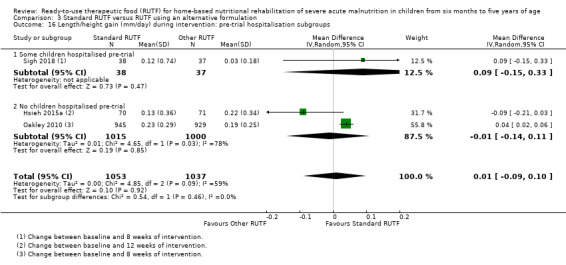
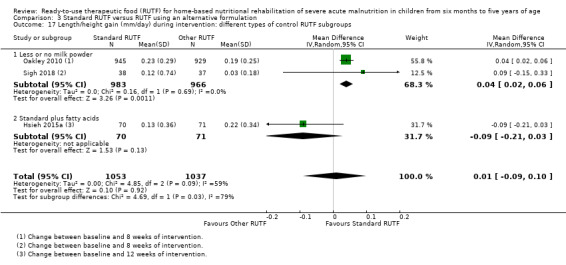
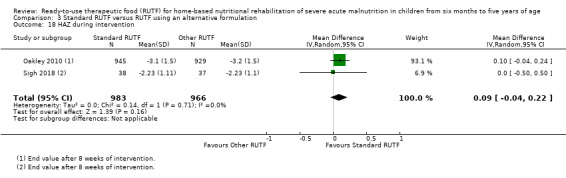
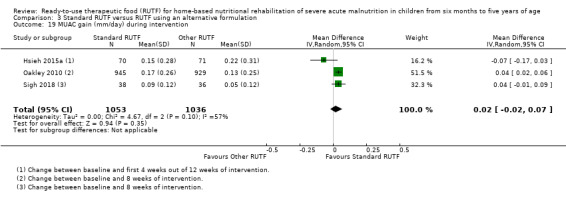
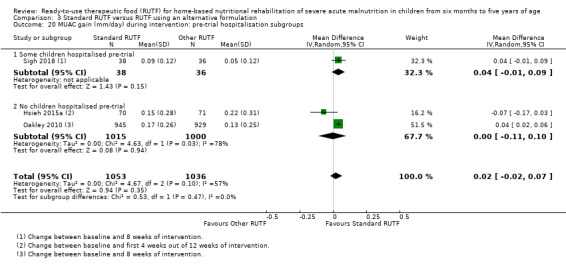
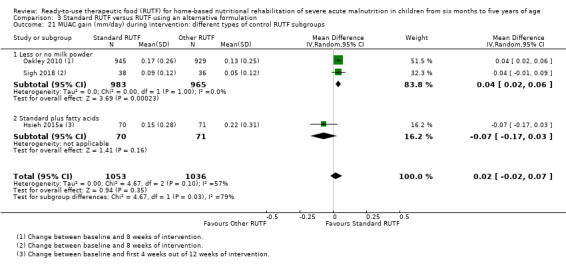
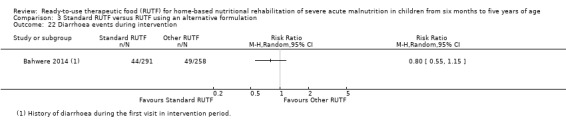
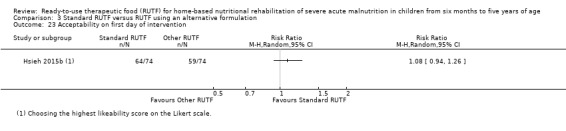
Main results: We included 15 eligible studies (n = 7976; effective sample size = 6630), four of which were cluster trials. Eight studies were conducted in Malawi, four in India, and one apiece in Kenya, Zambia, and Cambodia. Six studies received funding or donations from industry whereas eight did not, and one study did not report the funding source.The overall risk of bias was high for six studies, unclear for three studies, and low for six studies. Among the 14 studies that contributed to meta-analyses, none (n = 5), some (n = 5) or all (n = 4) children were stabilised in hospital prior to commencement of the study. One small study included only children known to be HIV-infected, another study stratified the analysis for 'recovery' according to HIV status, while the remaining studies included HIV-uninfected or untested children. Across all studies, the intervention lasted between 8 and 16 weeks. Only five studies followed up children postintervention (maximum of six months), and generally reported on a limited number of outcomes.We found seven studies with 2261 children comparing home-based RUTF meeting the World Health Organization (WHO) recommendations for nutritional composition (referred to in this review as standard RUTF) with an alternative dietary approach (effective sample size = 1964). RUTF probably improves recovery (risk ratio (RR) 1.33; 95% confidence interval (CI) 1.16 to 1.54; 6 studies, 1852 children; moderate-quality evidence), and may increase the rate of weight gain slightly (mean difference (MD) 1.12 g/kg/day, 95% CI 0.27 to 1.96; 4 studies, 1450 children; low-quality evidence), but we do not know the effects on relapse (RR 0.55, 95% CI 0.30 to 1.01; 4 studies, 1505 children; very low-quality evidence) and mortality (RR 1.05, 95% CI 0.51 to 2.16; 4 studies, 1505 children; very low-quality evidence).Two quasi-randomised cluster trials compared standard, home-based RUTF meeting total daily nutritional requirements with a similar RUTF but given as a supplement to the usual diet (213 children; effective sample size = 210). Meta-analysis showed that standard RUTF meeting total daily nutritional requirements may improve recovery (RR 1.41, 95% CI 1.19 to 1.68; low-quality evidence) and reduce relapse (RR 0.11, 95% CI 0.01 to 0.85; low-quality evidence), but the effects are unknown for mortality (RR 1.36, 95% CI 0.46 to 4.04; very low-quality evidence) and rate of weight gain (MD 1.21 g/kg/day, 95% CI - 0.74 to 3.16; very low-quality evidence).Eight studies randomised 5502 children (effective sample size = 4456) and compared standard home-based RUTF with RUTFs of alternative formulations (e.g. using locally available ingredients, containing less or no milk powder, containing specific fatty acids, or with added pre- and probiotics). For recovery, it made little or no difference whether standard or alternative formulation RUTF was used (RR 1.03, 95% CI 0.99 to 1.08; 6 studies, 4188 children; high-quality evidence). Standard RUTF decreases relapse (RR 0.84, 95% CI 0.72 to 0.98; 6 studies, 4188 children; high-quality evidence). However, it probably makes little or no difference to mortality (RR 1.00, 95% CI 0.80 to 1.24; 7 studies, 4309 children; moderate-quality evidence) and may make little or no difference to the rate of weight gain (MD 0.11 g/kg/day, 95% CI -0.32 to 0.54; 6 studies, 3807 children; low-quality evidence) whether standard or alternative formulation RUTF is used.
Authors' conclusions: Compared to alternative dietary approaches, standard RUTF probably improves recovery and may increase rate of weight gain slightly, but the effects on relapse and mortality are unknown. Standard RUTF meeting total daily nutritional requirements may improve recovery and relapse compared to a similar RUTF given as a supplement to the usual diet, but the effects on mortality and rate of weight gain are not clear. When comparing RUTFs with different formulations, the current evidence does not favour a particular formulation, except for relapse, which is reduced with standard RUTF. Well-designed, adequately powered, pragmatic RCTs with standardised outcome measures, stratified by HIV status, and that include diarrhoea as an outcome, are needed.
Conflict of interest statement
Anel Schoonees ‐ none known
Martani Lombard ‐ none known
Alfred Musekiwa ‐ none known
Etienne Nel has received honoraria from the following organisations in 2018 for lectures given:
AbbVie. Topic: Crohn’s Disease in Children
Nestle Nutrition Institute in Africa. Topic: Human Milk Oligosaccharides
Cipla. Topic: Constipation in Children
Jimmy Volmink ‐ none known
Figures

Update of
-
Ready-to-use therapeutic food for home-based treatment of severe acute malnutrition in children from six months to five years of age.Cochrane Database Syst Rev. 2013 Jun 6;2013(6):CD009000. doi: 10.1002/14651858.CD009000.pub2. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2019 May 15;5:CD009000. doi: 10.1002/14651858.CD009000.pub3. PMID: 23744450 Free PMC article. Updated.
References
References to studies included in this review
Bahwere 2014 {published and unpublished data}
-
- Bahwere P, Banda T, Sadler K, Nyirenda G, Owino V, Shaba B, et al. Effectiveness of milk whey protein‐based ready‐to‐use therapeutic food in treatment of severe acute malnutrition in Malawian under‐5 children: a randomised, double‐blind, controlled non‐inferiority clinical trial. Maternal & Child Nutrition 2014;10(3):436‐51. [DOI: 10.1111/mcn.12112; PUBMED: 24521353] - DOI - PMC - PubMed
Bhandari 2016 {published data only}
-
- Bhandari N, Mohan SB, Bose A, Iyengar SD, Taneja S, Mazumder S, et al. Efficacy of three feeding regimens for home‐based management of children with uncomplicated severe acute malnutrition: a randomised trial in India. BMJ Global Health 2016;1(4):e000144. [DOI: 10.1136/bmjgh-2016-000144] - DOI - PMC - PubMed
Ciliberto 2005 {published and unpublished data}
-
- Ciliberto MA, Sandige H, Ndekha MJ, Ashorn P, Briend A, Ciliberto HM, et al. Comparison of home‐based therapy with ready‐to‐use therapeutic food with standard therapy in the treatment of malnourished Malawian children: a controlled, clinical effectiveness trial. American Journal of Clinical Nutrition 2005;81(4):864‐70. [DOI: 10.1093/ajcn/81.4.864; PUBMED: 15817865] - DOI - PubMed
Hsieh 2015a {published data only}
-
- Hsieh J‐C, Liu L, Zeilani M, Ickes S, Trehan I, Maleta K, et al. High‐oleic ready‐to‐use therapeutic food maintains docosahexaenoic acid status in severe malnutrition. Journal of Pediatric Gastroenterology and Nutrition 2015;61(1):138‐43. [DOI: 10.1097/MPG.0000000000000741; PMC4483140; PUBMED: 25633498] - DOI - PMC - PubMed
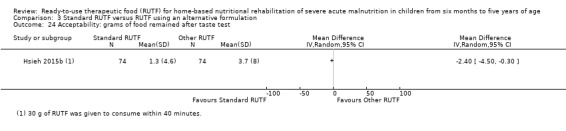
Hsieh 2015b {published and unpublished data}
-
- Hsieh J‐C, Liu L, Zeilani M, Ickes S, Trehan I, Maleta K, et al. High‐oleic ready‐to‐use therapeutic food maintains docosahexaenoic acid status in severe malnutrition. Journal of Pediatric Gastroenterology and Nutrition 2015;61(1):138‐43. [DOI: 10.1097/MPG.0000000000000741; PMC4483140; PUBMED: 25633498] - DOI - PMC - PubMed
Irena 2015 {published and unpublished data}
-
- Irena AH, Bahwere P, Owino VO, Diop EI, Bachmann MO, Mbwili‐Muleya C, et al. Comparison of the effectiveness of a milk‐free soy‐maize‐sorghum‐based ready‐to‐use therapeutic food to standard ready‐to‐use therapeutic food with 25% milk in nutrition management of severely acutely malnourished Zambian children: an equivalence non‐blinded cluster randomised controlled trial. Maternal & Child Nutrition 2015;11(Suppl 4):105‐19. [DOI: 10.1111/mcn.12054; PUBMED: 23782554] - DOI - PMC - PubMed
Jadhav 2016 {published and unpublished data}
-
- Jadhav A, Dias B, Shah N, Fernandes L, Fernandes S, Surve A, et al. A randomized controlled facility based trial to assess the impact of indigenously prepared ready to use therapeutic food (RUTF) for children with severe acute malnutrition in Inda. Pediatric Oncall 2016;13(4):93‐8. [DOI: 10.7199/ped.oncall.2016.61] - DOI
Jones 2015 {published data only}
-
- Jones KD, Ali R, Khasira MA, Odera D, West AL, Koster G, et al. Ready‐to‐use therapeutic food with elevated n‐3 polyunsaturated fatty acid content, with or without fish oil, to treat severe acute malnutrition: a randomized controlled trial. BMC Medicine 2015;13:93. [DOI: 10.1186/s12916-015-0315-6; PMC4407555; PUBMED: 25902844] - DOI - PMC - PubMed
Kerac 2009 {published and unpublished data}
-
- Kerac M. Improving the Treatment of Severe Acute Malnutrition in Childhood: A Randomized Controlled Trial of Synbiotic‐enhanced Therapeutic Food with Long Term Follow‐up of Post‐treatment Mortality and Morbidity [Doctoral thesis]. London (UK): University College London, 2011. [discovery.ucl.ac.uk/1306755/]
Manary 2004 {published and unpublished data}
Ndekha 2005 {published data only (unpublished sought but not used)}
-
- Ndekha MJ, Manary MJ, Ashorn P, Briend A. Home‐based therapy with ready‐to‐use therapeutic food is of benefit to malnourished, HIV‐infected Malawian children. Acta Paediatrica 2005;94(2):222‐5. [PUBMED: 15981758] - PubMed
Oakley 2010 {published and unpublished data}
-
- Oakley E, Reinking J, Sandige H, Trehan I, Kennedy G, Maleta K, et al. A ready‐to‐use therapeutic food containing 10% milk is less effective than one with 25% milk in the treatment of severely malnourished children. The Journal of Nutrition 2010;140(12):2248‐52. [DOI: 10.3945/jn.110.123828; PMC2981006; PUBMED: 20980648] - DOI - PMC - PubMed
Shewade 2013 {published data only}
-
- Shewade HD, Patro BK, Bharti B, Soundappan K, Kaur A, Taneja N. Effectiveness of indigenous ready‐to‐use therapeutic food in community‐based management of uncomplicated severe acute malnutrition: a randomized controlled trial from India. Journal of Tropical Pediatrics 2013;59(5):393‐8. [DOI: 10.1093/tropej/fmt039; PUBMED: 23751252] - DOI - PubMed
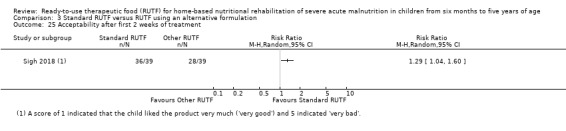
Sigh 2018 {unpublished data only}
-
- Sigh S, Roos N, Chamnan C, Laillou A, Prak S, Wieringa FT. Effectiveness of a locally produced, fish‐based food product on weight gain among Cambodian children in the treatment of acute malnutrition: a randomized controlled trial. Nutrients 2018;10(7):e909. [DOI: 10.3390/nu10070909; PMC6073612; PUBMED: 30012981] - DOI - PMC - PubMed
-
- Sigh S, Roos N, Sok D, Borg B, Chamnan C, Laillou A, et al. Development and acceptability of locally made fish‐based, ready‐to‐use products for the prevention and treatment of malnutrition in Cambodia. Food and Nutrition Bulletin 2018;39(3):420‐34. [DOI: 10.1177/0379572118788266; PUBMED: 30092653 ] - DOI - PubMed
Thapa 2017 {published data only}
-
- Thapa BR, Goyal P, Menon J, Sharma A. Acceptability and efficacy of locally produced ready‐to‐use therapeutic food Nutreal in the management of severe acute malnutrition in comparison with defined food. Food and Nutrition Bulletin 2017;38(1):18‐26. [DOI: 10.1177/0379572116689743; PUBMED: 28125907] - DOI - PubMed
References to studies excluded from this review
Amthor 2009 {published data only}
Ashraf 2017 {published data only}
-
- Ashraf M, Mahmood S, Chaudhry MA. Effect of F‐75, F‐100 and RUTF (ready to use therapeutic food) supplementation in children with severe malnutrition. Pakistan Journal of Medical & Health Sciences 2017;11(1):339‐42. [www.pjmhsonline.com/2017/jan_march/pdf/339.pdf]
Bahwere 2016 {published data only}
-
- Bahwere P, Balaluka B, Wells JC, Mbiribindi CN, Sadler K, Akomo P, et al. Cereals and pulse‐based ready‐to‐use therapeutic food as an alternative to the standard milk‐ and peanut paste‐based formulation for treating severe acute malnutrition: a noninferiority, individually randomized controlled efficacy clinical trial. American Journal of Clinical Nutrition 2016;103(4):1145‐61. [DOI: 10.3945/ajcn.115.119537; PUBMED: 26984485] - DOI - PubMed
Bahwere 2017 {published data only}
-
- Bahwere P, Akomo P, Mwale M, Murakami H, Banda C, Kathumba S, et al. Soya, maize, and sorghum–based ready‐to‐use therapeutic food with amino acid is as efficacious as the standard milk and peanut paste–based formulation for the treatment of severe acute malnutrition in children: a noninferiority individually randomized controlled efficacy clinical trial in Malawi. Americal Journal of Clinical Nutrition 2017;106(4):1100–12. [DOI: ; PUBMED: 28814393] - PubMed
Briend 1999 {published data only}
Brown 2015 {published data only}
Choudhury 2018 {published data only}
-
- Choudhury N, Ahmed T, Hossain I, Islam MM, Sarker SA, Zeilani M, et al. Ready‐to‐use therapeutic food made from locally available food ingredients is well accepted by children having severe acute malnutrition in Bangladesh. Food and Nutrition Bulletin 2018;39(1):116‐26. [DOI: 10.1177/0379572117743929; PUBMED: 29258336] - DOI - PubMed
CTRI/2013/02/003418 {published data only}
-
- CTRI/2013/02/003418. Effectiveness of ready to eat food in treating severely malnourished children in community settings, a study from Puducherry [Effectiveness of indigenous ready to use therapeutic food (RUTF) in community‐based management of uncomplicated severe acute malnutrition (SAM): a randomized trial from Puducherry, India]. www.ctri.nic.in/Clinicaltrials/pdf_generate.php?trialid=6017&EncHid=... (first received 21 February 2013).
Dani 2017 {published data only}
-
- Dani V, Satav K, Pendharkar J, Satav A, Ughade S, Adhav A, et al. Community‐based management of severe malnutrition: SAM and SUW in the tribal area of Melghat, Maharashtra, India. Clinical Epidemiology and Global Health 2017;5(2):62‐9. [DOI: 10.1016/j.cegh.2016.11.003] - DOI
Diop 2003 {published data only}
-
- Diop EH, Dossou NI, Ndour MM, Briend A, Wade S. Comparison of the efficacy of a solid ready‐to‐use food and a liquid, milk‐based diet for the rehabilitation of severely malnourished children: a randomized trial. American Journal of Clinical Nutrition 2003;78(2):302‐7. [DOI: 10.1093/ajcn/78.2.302; PUBMED: 12885713] - DOI - PubMed
Diop 2004 {published data only}
-
- Diop EI, Dossou NI, Briend A, Yaya MM, Ndour MM, Wade S. Home‐based rehabilitation for severely malnourished children using locally made ready‐to‐use therapeutic food (RTUF). Second World Congress of Pediatric Gastroenterology, Hepatology and Nutrition; 2004 Jul 3‐7; Paris (FR) 2004:101‐5.
Dube 2009 {published data only}
-
- Dube B, Rongsen T, Mazumder S, Taneja S, Rafiqui F, Bhandari N, et al. Comparison of ready‐to‐use therapeutic food with cereal legume‐based khichri among malnourished children. Indian Pediatrics 2009;46(5):383‐8. [PUBMED: 19179743] - PubMed
Greco 2006 {published data only}
Ige 2014 {published data only}
-
- Ige OK, Oladokun RE, Kikelomo O. Comparative weight gain with ready‐to‐use therapeutic food in stunted HIV‐infected and ‐uninfected children in a Nigerian Hospital. South African Journal of Child Health 2014;8(3):104‐7. [DOI: 10.7196/SAJCH.723] - DOI
Kuusipalo 2006 {published data only}
-
- Kuusipalo H, Maleta K, Briend A, Manary M, Ashorn P. Growth and change in blood haemoglobin concentration among underweight Malawian infants receiving fortified spreads for 12 weeks: a preliminary trial. Journal of Pediatric Gastroenterology and Nutrition 2006;43(4):525‐32. [DOI: 10.1097/01.mpg.0000235981.26700.d3; PUBMED: 17033530] - DOI - PubMed
Lagrone 2010 {published data only}
-
- Lagrone L, Cole S, Schondelmeyer A, Maleta K, Manary MJ. Locally produced ready‐to‐use supplementary food is an effective treatment of moderate acute malnutrition in an operational setting. Annals of Tropical Paediatrics 2010;30(2):103‐8. [DOI: 10.1179/146532810X12703901870651; PUBMED: 20522296] - DOI - PubMed
LaGrone 2012 {published data only}
-
- LaGrone LN, Trehan I, Meuli GJ, Wang RJ, Thakwalakwa C, Maleta K, et al. A novel fortified blended flour, corn‐soy blend "plus‐plus," is not inferior to lipid‐based ready‐to‐use supplementary foods for the treatment of moderate acute malnutrition in Malawian children. American Journal of Clinical Nutrition 2012;95(1):212‐9. [DOI: 10.3945/ajcn.111.022525; PMC3238461; PUBMED: 22170366] - DOI - PMC - PubMed
Linneman 2007 {published data only}
-
- Linneman Z, Matilsky D, Ndekha M, Manary MJ, Maleta K, Manary MJ. A large‐scale operational study of home‐based therapy with ready‐to‐use therapeutic food in childhood malnutrition in Malawi. Maternal & Child Nutrition 2007;3(3):206‐15. [DOI: 10.1111/j.1740-8709.2007.00095.x; PUBMED: 17539889] - DOI - PMC - PubMed
Lopriore 2004 {published data only}
Maleta 2004 {published data only}
-
- Maleta K, Kuittinen J, Duggan MB, Briend A, Manary M, Wales J, et al. Supplementary feeding of underweight, stunted Malawian children with ready‐to‐use food. Journal of Pediatric Gastroenterology and Nutrition 2004;38(2):152‐8. [PUBMED: 14734876] - PubMed
Malik 2016 {published and unpublished data}
-
- Malik S, Mittal M, Kushwaha KP. WHO/UNICEF recommended therapeutic food versus home based therapeutic food in the management of severe acute malnutrition: a randomized controlled trial. Sudanese Journal of Paediatrics 2016;16(2):21‐7. [PMC5237831; www.sudanjp.org; PUBMED: 28096555] - PMC - PubMed
Mallewa 2018 {published data only}
-
- Mallewa J, Szubert AJ, Mugyenyi P, Chidziva E, Thomason MJ, Chepkorir P, et al. Effect of ready‐to‐use supplementary food on mortality in severely immunocompromised HIV‐infected individuals in Africa initiating antiretroviral therapy (REALITY): an open‐label, parallel‐group, randomised controlled trial. Lancet HIV 2018;5(5):e231–40. [DOI: 10.1016/S2352-3018(18)30038-9; PMC5932190; PUBMED: 29653915] - DOI - PMC - PubMed
Mamidi 2011 {published data only}
-
- Mamidi RS, Kulkarni B, Radhakrishna KV. Hospital‐based nutrition rehabilitation of children with severe acute malnutrition ‐ experiences from a nutrition centre in India. Nutrition Therapy & Metabolism 2011;29(3):107‐18. [Issn Print: 0393‐5585; Ovid insights.ovid.com/nthme/201129030/01698830‐201129030‐00001]
Manary 2013 {published data only}
-
- Manary M. Protein source and quality in therapeutic foods affect the immune response and outcome in severe acute malnutrition. Food and Nutrition Bulletin 2013;34(2):256‐8. [PUBMED: 23964405] - PubMed
Matilsky 2009 {published data only}
-
- Matilsky DK, Maleta K, Castleman T, Manary MJ. Supplementary feeding with fortified spreads results in higher recovery rates than with a corn/soy blend in moderately wasted children. Journal of Nutrition 2009;139(4):773‐8. [DOI: 10.3945/jn.108.104018; PMC3151028; PUBMED: 19225128] - DOI - PMC - PubMed
Maust 2015 {published data only}
Nackers 2010 {published and unpublished data}
-
- Nackers F, Broillet F, Oumarou D, Djibo A, Gaboulaud V, Guerin PJ. Effectiveness of ready‐to‐use therapeutic food compared to a corn/soy‐blend‐based pre‐mix for the treatment of childhood moderate acute malnutrition in Niger. Journal of Tropical Pediatrics 2010;56(6):407‐13. [DOI: 10.1093/tropej/fmq019; PUBMED: 20332221] - DOI - PubMed
Navarro‐Colorado 2005 {published data only}
-
- Navarro‐Colorado C, Laquière S. Clinical trial of BP100 vs F100 milk for rehabilitation of severe malnutrition. Field Exchange 2005;24:22‐4. [www.ennonline.net/fex/24/clinical]
Nga 2013 {published data only}
-
- Nga TT, Nguyen M, Mathisen R, Hoa DT, Minh HN, Hop LT, et al. Effectiveness of a locally produced ready‐to‐use‐therapeutic food for the treatment of children with acute malnutrition in Vietnam. Annals of Nutrition & Metabolism 2013;63(Suppl 1):1084. [DOI: 10.1159/000354245; PO1727; www.karger.com/Article/Pdf/354245] - DOI
Patel 2005 {published data only}
-
- Patel MP, Sandige HL, Ndekha MJ, Briend A, Ashorn P, Manary MJ. Supplemental feeding with ready‐to‐use therapeutic food in Malawian children at risk of malnutrition. Journal of Health, Population and Nutrition 2005;23(4):351‐7. [PUBMED: 16599106] - PubMed
Phuka 2008 {published data only}
-
- Phuka JC, Maleta K, Thakwalakwa C, Cheung YB, Briend A, Manary MJ, et al. Complementary feeding with fortified spread and incidence of severe stunting in 6‐ to 18‐month‐old rural Malawians. Archives of Pediatrics & Adolescent Medicine 2008;162(7):619‐26. [DOI: 10.1001/archpedi.162.7.619; PMC3721756; PUBMED: 18606932] - DOI - PMC - PubMed
Sandige 2004 {published and unpublished data}
-
- Sandige H, Ndekha MJ, Briend A, Ashorn P, Manary MJ. Home‐based treatment of malnourished Malawian children with locally produced or imported ready‐to‐use food. Journal of Pediatric Gastroenterology and Nutrition 2004;39(2):141‐6. [PUBMED: 15269617] - PubMed
Sato 2018 {published data only}
-
- Sato W, Furuta C, Matsunaga K, Bahwere P, Collins S, Sadler K, et al. Amino‐acid‐enriched cereals ready‐to‐use therapeutic foods (RUTF) are as effective as milk‐based RUTF in recovering essential amino acid during the treatment of severe acute malnutrition in children: an individually randomized control trial in Malawi. PLoS ONE 2018;13(8):e0201686. [DOI: 10.1371/journal.pone.0201686; PMC6086422; PUBMED: 30096200] - DOI - PMC - PubMed
Singh 2010 {published data only}
-
- Singh AS, Kang G, Ramachandran A, Sarkar R, Peter P, Bose A. Locally made ready‐to‐use therapeutic food for treatment of malnutrition: a randomized controlled trial. Indian Pediatrics 2010;47(8):679‐86. [PUBMED: 20972285] - PubMed
Thakwalakwa 2010 {published data only}
-
- Thakwalakwa C, Ashorn P, Phuka J, Cheung YB, Briend A, Puumalainen T, et al. A lipid‐based nutrient supplement but not corn‐soy blend modestly increases weight gain among 6‐ to 18‐month‐old moderately underweight children in rural Malawi. Journal of Nutrition 2010;140(11):2008‐13. - PubMed
Van Hoan 2009 {published data only}
Wasnik 2012 {published data only}
-
- Wasnik VR, Rathi M. Effect of locally made ready‐to‐use therapeutic food (mushpro health drink powder – MHDP) for treatment of malnutrition on children aged 6 to 72 months in tribal area of Amravati district of Maharashtra, India: a randomized control trial. International Journal of Collaborative Research on Internal Medicine & Public Health 2012;4(7):1472‐87. [internalmedicine.imedpub.com/effect‐of‐locally‐made‐readytouse‐therapeut...
References to studies awaiting assessment
Huq 2013 {published data only}
-
- Huq S, Hossain MI, Islam MM, Ahmed T. Acceptability and efficacy of ready‐to‐use therapeutic food in 6‐24 months old children with severe acute malnutrition in Bangladesh. Annals of Nutrition & Metabolism 2013;63(Suppl 1):309. [DOI: 10.1159/000354245; PO109] - DOI
Kaleem 2014 {published data only}
-
- Kaleem R, Aziz N, Zaman S, Salimi MA. Nutritional rehabilitation of severely malnourished children by high density diet in comparison to ready to use therapeutic food. Pakistan Paediatric Journal 2014;38(4):235‐43. [ISSN 2305‐820X; www.pakmedinet.com/22343]
References to ongoing studies
CTRI/2014/09/004958 {published data only}
-
- CTRI/2014/09/004958. To establish effective nutrition protocol for community based management of children with severe acute malnutrition and to demonstrate operational feasibility through the existing Government system in Nandurbar district of Maharashtra in India [Community based management of acute malnutrition (CMAM) using global protocol ‐ MNT/RUTF in Nandurbar ‐ CMAM]. apps.who.int/trialsearch/Trial2.aspx?trialid=CTRI/2014/09/004958 (first received 2 September 2014). [www.ctri.nic.in/Clinicaltrials/pmaindet2.php?trialid=10011]
CTRI/2016/02/006656 {published data only}
-
- CTRI/2016/02/006656. Gut inflammation markers as determinants of response to recovery in uncomplicated severely malnourished children [Gut inflammation markers as determinants of response to treatment and recovery in children with uncomplicated severe acute malnutrition undergoing community based rehabilitation ‐ gut markers predictor of recovery in SAM children]. apps.who.int/trialsearch/Trial2.aspx?trialid=CTRI/2016/02/006656 (first received 17 February 2016). [www.ctri.nic.in/Clinicaltrials/pmaindet2.php?trialid=7346]
ISRCTN30393230 {published data only}
-
- Bailey J, Lelijveld N, Marron B, Onyoo P, Ho LS, Manray M, et al. Combined protocol for acute malnutrition study (ComPAS) in rural South Sudan and urban Kenya: study protocol for a randomized controlled trial. Trials 2018;19(1):251. [DOI: 10.1186/s13063-018-2643-2; PMC5978994; PUBMED: 29690916] - DOI - PMC - PubMed
-
- ISRCTN30393230. Combined protocol for acute malnutrition study (ComPAS) [Combined protocol for acute malnutrition study (ComPAS) ‐ effectiveness of a combined and simplified protocol for the treatment of acute malnutrition: a prospective, multi‐center cluster‐randomized controlled non‐inferiority trial in Kenya and South Sudan]. www.isrctn.com/ISRCTN30393230?q=&filters=recruitmentCountry:South%20... (first received 18 January 2017). [DOI: 10.1186/ISRCTN30393230] - DOI
-
- Lelijveld N, Bailey J, Mayberry A, Trenouth L, N’Diaye DS, Haghparast‐Bidgoli H, et al. The "ComPAS Trial" combined treatment model for acute malnutrition: study protocol for the economic evaluation. Trials 2018;19(1):252. [DOI: 10.1186/s13063-018-2594-7; PMC5916722; PUBMED: 29690899] - DOI - PMC - PubMed
ISRCTN31143316 {unpublished data only}
-
- ISRCTN31143316. Treatment of severe acute malnutrition delivered by community health workers in Niger [A cohort study comparing treatment for severe acute malnutrition (SAM) in children between 6‐59 months, delivered by community health workers (CHWs) compared to a traditional facility based model in Mayahi district, Niger]. www.isrctn.com/ISRCTN31143316 (first received 31 July 2018). [10.1186/ISRCTN31143316]
ISRCTN50039021 {published data only}
-
- ISRCTN50039021. Modelling an alternative nutrition protocol generalizable for outpatient (MANGO) [Modelling an alternative nutrition protocol generalizable for outpatient (MANGO) ‐ effectiveness of an optimized dosage of RUTF for the treatment of severe acute malnutrition: a randomized controlled, non‐inferiority trial in Burkina Faso]. www.isrctn.com/ISRCTN50039021 (first received 13 April 2016). [DOI: 10.1186/ISRCTN50039021] - DOI
NCT00131417 {unpublished data only}
-
- NCT00131417. Ready to use therapeutic food in the rehabilitation of severely malnourished children [Comparison of the efficacy of a ready‐to‐use therapeutic food with a milk‐based diet in the rehabilitation of severely malnourished Ugandan children]. www.clinicaltrials.gov/ct2/show/NCT00131417 (first received 17 August 2005).
NCT00941434 {unpublished data only}
-
- NCT00941434. Community based management of malnutrition [Community based management of malnutrition. A proposal for Pakistan initiative for mothers and newborns]. www.clinicaltrials.gov/ct2/show/NCT00941434 (first received 16 July 2009).
NCT01144806 {unpublished data only}
-
- NCT01144806. Evaluation of energy expenditure, body composition and recovery rates in children with severe acute malnutrition [Evaluation of energy expenditure, body composition and recovery rates in children with severe acute malnutrition (SAM) receiving community‐based nutritional rehabilitation therapy]. www.clinicaltrials.gov/show/NCT01144806 (first received 15 June 2010).
NCT01331044 {published data only}
-
- NCT01331044. Ready to use therapeutic food (RUTF) in severe malnourished children (RUTF) [Efficacy and acceptability of ready to use therapeutic food (RUTF) in children aged 6‐24 months with severe acute malnutrition in Bangladesh]. clinicaltrials.gov/ct2/show/NCT01331044 (first received 6 April 2011).
NCT01634009 {unpublished data only}
-
- NCT01634009. Soy‐ready to use therapeutic food (RUTF) in severely malnourished children [Efficacy of ready to use therapeutic food using soy protein isolate in under‐5 children with severe acute malnutrition in Bangladesh]. www.clinicaltrials.gov/ct2/show/NCT01634009 (first received 12 June 2012).
NCT03094247 {published data only}
-
- NCT03094247. Feeding malnourished children different types of fatty acids to promote neurocognitive development [Improved polyunsaturated ready‐to‐use therapeutic food for improved neurocognitive outcomes in severe acute malnutrition]. clinicaltrials.gov/ct2/show/NCT03094247 (first received 23 March 2017).
NCT03407326 {unpublished data only}
-
- NCT03407326. Comparison of an alternative therapeutic food for the international food aid market to a standard ready‐to‐use therapeutic food (RUTF) for the treatment of severe acute malnutrition in children [Comparison of an alternative therapeutic food for the international food aid market to a standard ready‐to‐use therapeutic food (RUTF) for the treatment of severe acute malnutrition in children of the Western Rural Region and Pujehun District of Sierra Leone]. clinicaltrials.gov/ct2/show/NCT03407326 (first received 16 January 2018).
Additional references
Action Against Hunger 2009
-
- Action against hunger. Acute malnutrition: a preventable pandemic. www.actionagainsthunger.org/sites/default/files/publications/Acute_Malnu... (accessed 20 May 2013).
Akparibo 2017
-
- Akparibo R, Harris J, Blank L, Campbell MJ, Holdsworth M. Severe acute malnutrition in children aged under 5 years can be successfully managed in a non‐emergency routine community healthcare setting in Ghana. Maternal & Child Nutrition 2017;13(4):e12417. [DOI: 10.1111/mcn.12417; MEDLINE: ] - DOI - PMC - PubMed
Ashworth 2003
-
- Ashworth A, Khanum S, Jackson A, Schofield C. Guidelines for the inpatient treatment of severely malnourished children. www.who.int/nutrition/publications/guide_inpatient_text.pdf (accessed 2 November 2017).
Bachmann 2009
Balhara 2017
-
- Balhara KS, Silvestri DM, Winders WT, Selvam A, Kivlehan SM, Becker TK, et al. Impact of nutrition interventions on pediatric mortality and nutrition outcomes in humanitarian emergencies: a systematic review. Tropical Medicine & International Health 2017;22(12):1464‐92. [DOI: 10.1111/tmi.12986; PUBMED: 28992388] - DOI - PubMed
Bazzano 2017
-
- Bazzano AN, Potts KS, Bazzano LA, Mason JB. The life course implications of ready to use therapeutic food for children in low‐income countries. International Journal of Environmental Research and Public Health 2017;14(4):403. [DOI: 10.3390/ijerph14040403; PMC5409604; PUBMED: 28398257] - DOI - PMC - PubMed
Black 2008
Black 2013
Brewster 2006
Collins 2002
Collins 2003
Collins 2004
-
- Collins S, Henry J. Alternative RUTF formulations (special supplement 2). Community‐based Therapeutic Care 2004;Suppl 2:35. [www.ennonline.net/fex/102/4‐3‐2]
Collins 2006a
Collins 2006b
Covidence [Computer program]
-
- Veritas Health Innovation. Covidence. Version accessed 27 February 2019. Melbourne, Australia: Veritas Health Innovation.
DFID 2009
-
- Department for International Development (DFID). The Neglected Crisis of Undernutrition: Evidence for Action. London (UK): Department for International Development, 2009.
Fleet 2017
-
- Fleet A. Product specifications sheet: RUTF biscuit (BP100) (Version 2.0). www.unicef.org/supply/files/RUTF_Biscuit_BP‐100_UNICEF_specs.pdf (accessed 17 November 2017).
Frankenburg 1992
-
- Frankenburg W, Dodds J, Archer P, Shapiro H, Bresnick B. The Denver II: a major revision and restandardization of the Denver Developmental Screening Test. Pediatrics 1992;89(1):91‐7. - PubMed
Gabouland 2007
-
- Gabouland V, Dan‐Bouzoua N, Brasher C, Fedida G, Gergonne B, Brown V. Could nutritional rehabilitation at home complement or replace centre‐based therapeutic feeding programmes for severe malnutrition?. Journal of Tropical Paediatrics 2007;53(1):49‐51. [DOI: 10.1093/tropej/fml052; PUBMED: 17030533] - DOI - PubMed
Garg 2018
-
- Garg CC, Mazumder S, Taneja S, Shekhar M, Mohan SB, Bose A, et al. Costing of three feeding regimens for home‐based management of children with uncomplicated severe acute malnutrition from a randomised trial in India. BMJ Global Health 2018;3:e000702. [DOI: 10.1136/bmjgh-2017-000702] - DOI - PMC - PubMed
Gera 2010
-
- Gera T. Efficacy and safety of therapeutic nutrition products for home based therapeutic nutrition for severe acute malnutrition: a systematic review. Indian Pediatrics 2010;47(8):709‐18. [PUBMED: 20972288] - PubMed
Gera 2017
-
- Gera T, Pena‐Rosas JP, Boy‐Mena E, Sachdev HS. Lipid based nutrient supplements (LNS) for treatment of children (6 months to 59 months) with moderate acute malnutrition (MAM): a systematic review. PLoS One 2017;12(9):e0182096. [DOI: 10.1371/journal.pone.0182096; PMC5608196; PUBMED: 28934235] - DOI - PMC - PubMed
GRADEPro GDT 2015 [Computer program]
-
- McMaster University (developed by Evidence Prime). GradePro GDT. Version (accessed 27 February 2019). Hamilton (ON): McMaster University (developed by Evidence Prime), 2015.
Greiner 2014
-
- Greiner T. Breastfeeding Briefs N° 56/57, September 2014. The advantages, disadvantages and risks of ready‐to‐use foods. ibfan.org/breastfeedingbreafs/BB%2056‐57‐The%20advantages‐disadvantages‐... (accessed 4 August 2017).
Grellety 2000
-
- Grellety Y. Management of Severe Malnutrition in Africa [PhD thesis]. Aberdeen (UK): University of Aberdeen, 2000.
Guyatt 2011
Hamil 1979
Hawkes 2015
-
- Hawkes C, Haddad L, Udomkesmalee E, Co‐Chairs of the Independent Expert Group of the Global Nutrition Report. The Global Nutrition Report 2015: what we need to do to advance progress in addressing malnutrition in all its forms. Public Health Nutrition 2015;18(17):3067‐9. [DOI: 10.1017/S1368980015003158; PUBMED: 26551284] - DOI - PMC - PubMed
Heikens 2008
Higgins 2002
Higgins 2003
Higgins 2011
-
- Higgins JP, Deeks JJ, Altman DG, editor(s). Chapter 16: Special topics in statistics. In: Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Higgins 2017
-
- Higgins JP, Altman DG, Sterne JA, editor(s). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS , editor(s). Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017). Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Hoffmann 2017
Hoskens 2018
-
- Hoskens J, Klingels K, Smits‐Engelsman B. Validity and cross‐cultural differences of the Bayley Scales of Infant and Toddler Development, Third Edition in typically developing infants. Early Human Development 2018;25:17‐25. - PubMed
Iannotti 2015
Isanaka 2009
-
- Isanaka S, Nombela N, Djibo A, Poupard M, Beckhoven D, Gabouland V, et al. Effect of preventive supplementation with ready‐to‐use therapeutic food on the nutritional status, mortality, and morbidity of children aged 6 to 60 months in Niger: a cluster randomized trial. JAMA 2009;301(3):277‐85. [DOI: 10.1001/jama.2008.1018; PMC3144630; NCT00682708; PUBMED: 19155454] - DOI - PMC - PubMed
Isanaka 2017
James 2015
-
- James PT, Briel N, Rozet A, Israël AD, Fenn B, Navarro‐Colorado C. Low‐dose RUTF protocol and improved service delivery lead to good programme outcomes in the treatment of uncomplicated SAM: a programme report from Myanmar. Maternal & Child Nutrition 2015;11(4):859‐69. [DOI: 10.1111/mcn; PMC4672709; PUBMED: 25850698] - DOI - PMC - PubMed
Jayatissa 2012
Jones 2014
Kabalo 2017
-
- Kabalo MY, Seifu CN. Treatment outcomes of severe acute malnutrition in children treated within Outpatient Therapeutic Program (OTP) at Wolaita Zone, Southern Ethiopia: retrospective cross‐sectional study. Journal of Health, Population and Nutrition 2017;36(1):7. [DOI: 10.1186/s41043-017-0083-3; PMC5345228; PUBMED: 28279227] - DOI - PMC - PubMed
Kassebaum 2017
-
- The Global Burden of Disease Child and Adolescent Health Collaboration. Child and adolescent health from 1990 to 2015 findings from the Global Burden of Diseases, Injuries, and Risk factors 2015 study. JAMA Pediatrics 2017;171(6):573‐92. [DOI: 10.1001/jamapediatrics.2017.0250; PMC5540012; PUBMED: 28384795] - DOI - PMC - PubMed
Komrska 2010a
-
- Komrska J. UNICEF requirements for RUTF manufacturers. www.unicef.org/supply/files/Technical_Requirements_for_RUTF_Manufacturer... (accessed 4 August 2017).
Komrska 2010b
-
- Komrska J. Overview of UNICEF’s RUTF procurement in 2010 and past years. www.unicef.org/supply/files/Overview_of_UNICEF_RUTF_Procurement_in_2010.pdf (accessed 4 August 2017).
Kruger 2008
-
- Kruger HS, Hendricks M, Puoane T. Nutritional management of multiple nutrient deficiencies. In: Steyn NP, Temple NJ editor(s). Community Nutrition Textbook for South Africa: A Rights‐Based Approach. Tygerberg (ZA): Chronic Diseases of Lifestyle Unit, Medical Research Council, 2008:674‐9.
Lazzerini 2012
Lazzerini 2013
Lenters 2013
-
- Lenters LM, Wazny K, Webb P, Ahmed T, Bhutta ZA. Treatment of severe and moderate acute malnutrition in low‐ and middle‐income settings: a systematic review, meta‐analysis and Delphi process. BMC Public Health 2013;13(Suppl 3):S23. [DOI: 10.1186/1471-2458-13-S3-S23; PMC3847503 ; PUBMED: 24564235] - DOI - PMC - PubMed
Lin 2008
Manary 2006
Manary 2008
Manary 2016
Mody 2014
Moher 2009
-
- Moher D, Liberati A, Tetzlaff J, Altman DG, the PRISMA Group. Preferred reporting items for systematic reviews and meta‐analyses: the PRISMA Statement. Annals of Internal Medicine 2009;151:264‐9. - PubMed
Moss 2006
-
- Moss WJ, Ramakrishnan M, Storms D, Henderson Siegle A, Weiss WM, Lejnev I, et al. Child health in complex emergencies. Bulletin of the World Health Organization 2006;84:58‐64. [www.who.int/hac/techguidance/pht/Child_health_in_emergencies.pdf] - PMC - PubMed
Naude 2008
-
- Naude CE, Labuschange IL, Labadarios D. Nutritional management of HIV/AIDS and TB. In: Steyn NP, Temple NJ editor(s). Community Nutrition Textbook for South Africa: A Rights‐Based Approach. Tygerberg (ZA): Chronic Diseases of Lifestyle Unit, Medical Research Council, 2008:751‐94.
Puett 2013
-
- Puett C, Sadler K, Alderman H, Coates J, Fiedler JL, Myatt M. Cost‐effectiveness of the community‐based management of severe acute malnutrition by community health workers in southern Bangladesh. Health Policy and Planning 2013;28(4):386‐99. [DOI: 10.1093/heapol/czs070; PUBMED: 22879522] - DOI - PubMed
Review Manager 2014 [Computer program]
-
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Rogers 2018
-
- Rogers E, Martínez K, Morán JL, Alé FG, Charle P, Guerrero S, et al. Cost‐effectiveness of the treatment of uncomplicated severe acute malnutrition by community health workers compared to treatment provided at an outpatient facility in rural Mali. Human Resources for Health 2018;16(1):12. [DOI: 10.1186/s12960-018-0273-0; PMC5819265; PUBMED: 29458382] - DOI - PMC - PubMed
Sanghvi 2014
Seal 2007
-
- Seal A, Kerac M. Operational implications of using 2006 World Health Organization growth standards in nutrition programmes: secondary data analysis. BMJ 2007;334:733‐8. [DOI: 10.1136/bmj.39101.664109.AE] - DOI - PMC - PubMed
Segré 2017
Shea 2017
Shewade 2017 [pers comm]
-
- Shewade HD. CTRI/2013/02/003418 [personal communication]. Email to: A Schoonees 1 August 2017.
Simpore 2006
Sinclair 2012
Sterne 2017
-
- Sterne JA, Egger M, Moher D, Boutron I (editors). Chapter 10: Addressing reporting biases. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS (editors), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017), Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Tekeste 2012
-
- Tekeste A, Wondafrash M, Azene G, Deribe K. Cost effectiveness of community‐based and in‐patient therapeutic feeding programs to treat severe acute malnutrition in Ethiopia. Cost Effectiveness and Resource Allocation 2012;10:4. [DOI: 10.1186/1478-7547-10-4; PMC3323427; PUBMED: 22429892] - DOI - PMC - PubMed
Trehan 2015
UNICEF 2013a
-
- United Nations Children’s Fund (UNICEF). Improving child nutrition: the achievable imperative for global progress. www.unicef.org/publications/files/Nutrition_Report_final_lo_res_8_April.pdf (accessed 1 August 2018).
UNICEF 2013b
-
- United Nations Children's Fund (UNICEF). Ready‐to‐use therapeutic food for children with severe acute malnutrition. www.unicef.org/media/files/Current_Issues_Paper_‐_Ready_To_Use_Therapeut... (accessed 4 August 2017).
UNICEF 2013c
-
- United Nations Children's Fund (UNICEF) Evaluation Office. Evaluation of community management of acute malnutrition: global synthesis report. www.unicef.org/evaldatabase/files/Final_CMAM_synthesis_FINAL_VERSION_wit... (accessed 11 August 2017).
UNICEF 2015a
-
- United Nations Children’s Fund (UNICEF). Management of severe acute malnutrition in children: working towards results at scale. www.childrenandaids.org/sites/default/files/2017‐05/SAM%20Guidance.pdf (accessed 4 August 2017).
UNICEF 2015b
-
- United Nations Children’s Fund (UNICEF) Supply Division. Ready‐to‐use therapeutic food demand. www.unicef.org/supply/files/UNICEF_RUTF_Demand.pdf (accessed 11 August 2017).
UNICEF/WHO/WBG 2017
-
- United Nations Children’s Fund, World Health Organization, World Bank Group. Levels and trends in child malnutrition. www.who.int/nutgrowthdb/jme_brochoure2017.pdf?ua=1 (accessed 4 August 2017).
Weber 2016
WHO 2006
-
- World Health Organization. The WHO child growth standards. www.who.int/childgrowth/en/ (accessed 30 November 2017).
WHO 2008
-
- World Health Organization (WHO). Training course on child growth assessment: WHO child growth standards. www.who.int/childgrowth/training/module_c_interpreting_indicators.pdf (accessed 8 November 2017).
WHO 2012
-
- World Health Organization (WHO). Technical note: supplementary foods for the management of moderate acute malnutrition in infants and children 6–59 months of age. apps.who.int/iris/bitstream/10665/75836/1/9789241504423_eng.pdf?ua=1&... (accessed 4 August 2017).
WHO 2013
-
- World Health Organization (WHO). Guideline: updates on the management of severe acute malnutrition in infants and children. apps.who.int/iris/bitstream/10665/95584/1/9789241506328_eng.pdf (accessed 18 September 2017). - PubMed
WHO 2017a
-
- World Health Organization (WHO). Ambition and action in nutrition 2016–2025. www.who.int/nutrition/publications/nutrition‐strategy‐2016to2025/en/ (accessed 11 August 2017).
WHO 2017b
-
- World Health Organization (WHO). Management of severe acute malnutrition in infants and children. www.who.int/elena/titles/full_recommendations/sam_management/en/ (accessed 8 November 2017). - PubMed
WHO/UNICEF 2009
-
- World Health Organization, United Nations Children's Fund. WHO child growth standards and the identification of severe acute malnutrition in infants and children: a joint statement. www.who.int/nutrition/publications/severemalnutrition/9789241598163/en/i... (accessed 20 May 2013). - PubMed
WHO/WFP/UNSCN/UNICEF 2007
-
- World Health Organization, World Food Programme, United Nations System Standing Committee on Nutrition (UNSCN), United Nations Children's Fund (UNICEF). Community‐based management of severe acute malnutrition. www.who.int/nutrition/topics/Statement_community_based_man_sev_acute_mal... (accessed 20 May 2013).
References to other published versions of this review
Schoonees 2011
-
- Schoonees A, Lombard M, Nel E, Volmink J. Ready‐to‐use therapeutic food for treating undernutrition in children from 6 months to 5 years of age. Cochrane Database of Systematic Reviews 2011, Issue 2. [DOI: 10.1002/14651858.CD009000] - DOI
Schoonees 2013
-
- Schoonees A, Lombard M, Musekiwa A, Nel E, Volmink J. Ready‐to‐use therapeutic food for home‐based treatment of severe acute malnutrition in children from six months to five years of age. Cochrane Database of Systematic Reviews 2013, Issue 6. [DOI: 10.1002/14651858.CD009000.pub2] - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous