

Cardiovascular disease risk prediction using automated machine learning: A prospective study of 423,604 UK Biobank participants
- PMID: 31091238
- PMCID: PMC6519796
- DOI: 10.1371/journal.pone.0213653
Cardiovascular disease risk prediction using automated machine learning: A prospective study of 423,604 UK Biobank participants
Abstract
Background: Identifying people at risk of cardiovascular diseases (CVD) is a cornerstone of preventative cardiology. Risk prediction models currently recommended by clinical guidelines are typically based on a limited number of predictors with sub-optimal performance across all patient groups. Data-driven techniques based on machine learning (ML) might improve the performance of risk predictions by agnostically discovering novel risk predictors and learning the complex interactions between them. We tested (1) whether ML techniques based on a state-of-the-art automated ML framework (AutoPrognosis) could improve CVD risk prediction compared to traditional approaches, and (2) whether considering non-traditional variables could increase the accuracy of CVD risk predictions.
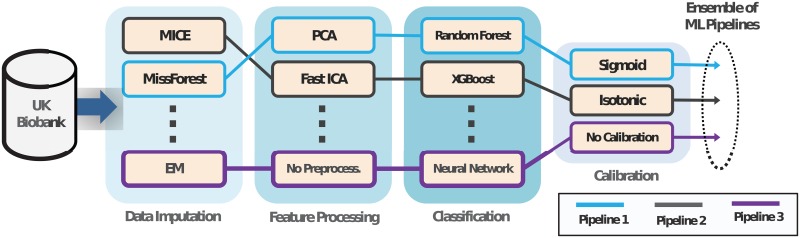
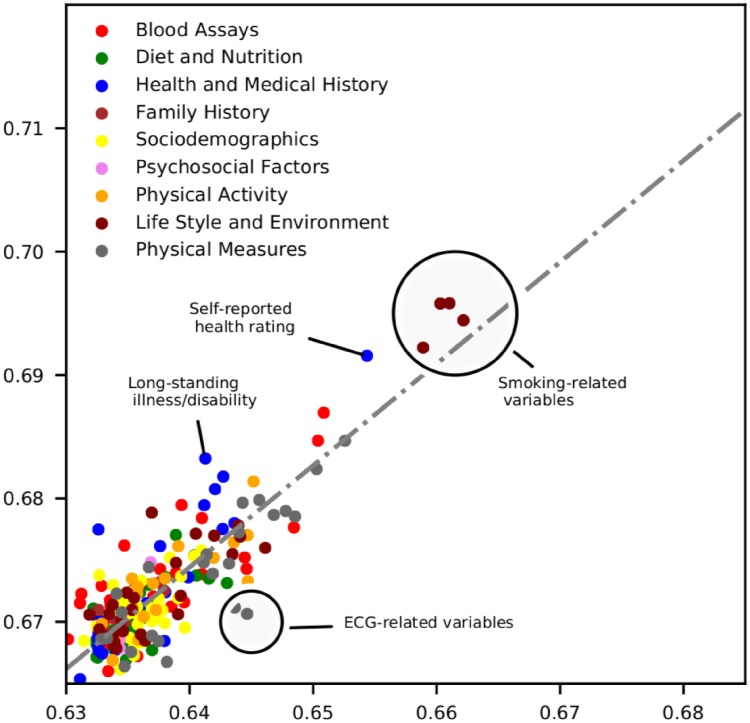
Methods and findings: Using data on 423,604 participants without CVD at baseline in UK Biobank, we developed a ML-based model for predicting CVD risk based on 473 available variables. Our ML-based model was derived using AutoPrognosis, an algorithmic tool that automatically selects and tunes ensembles of ML modeling pipelines (comprising data imputation, feature processing, classification and calibration algorithms). We compared our model with a well-established risk prediction algorithm based on conventional CVD risk factors (Framingham score), a Cox proportional hazards (PH) model based on familiar risk factors (i.e, age, gender, smoking status, systolic blood pressure, history of diabetes, reception of treatments for hypertension and body mass index), and a Cox PH model based on all of the 473 available variables. Predictive performances were assessed using area under the receiver operating characteristic curve (AUC-ROC). Overall, our AutoPrognosis model improved risk prediction (AUC-ROC: 0.774, 95% CI: 0.768-0.780) compared to Framingham score (AUC-ROC: 0.724, 95% CI: 0.720-0.728, p < 0.001), Cox PH model with conventional risk factors (AUC-ROC: 0.734, 95% CI: 0.729-0.739, p < 0.001), and Cox PH model with all UK Biobank variables (AUC-ROC: 0.758, 95% CI: 0.753-0.763, p < 0.001). Out of 4,801 CVD cases recorded within 5 years of baseline, AutoPrognosis was able to correctly predict 368 more cases compared to the Framingham score. Our AutoPrognosis model included predictors that are not usually considered in existing risk prediction models, such as the individuals' usual walking pace and their self-reported overall health rating. Furthermore, our model improved risk prediction in potentially relevant sub-populations, such as in individuals with history of diabetes. We also highlight the relative benefits accrued from including more information into a predictive model (information gain) as compared to the benefits of using more complex models (modeling gain).
Conclusions: Our AutoPrognosis model improves the accuracy of CVD risk prediction in the UK Biobank population. This approach performs well in traditionally poorly served patient subgroups. Additionally, AutoPrognosis uncovered novel predictors for CVD disease that may now be tested in prospective studies. We found that the "information gain" achieved by considering more risk factors in the predictive model was significantly higher than the "modeling gain" achieved by adopting complex predictive models.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
