

Sex Differences Persist in Time to Presentation, Revascularization, and Mortality in Myocardial Infarction Treated With Percutaneous Coronary Intervention
- PMID: 31092091
- PMCID: PMC6585344
- DOI: 10.1161/JAHA.119.012161
Sex Differences Persist in Time to Presentation, Revascularization, and Mortality in Myocardial Infarction Treated With Percutaneous Coronary Intervention
Abstract
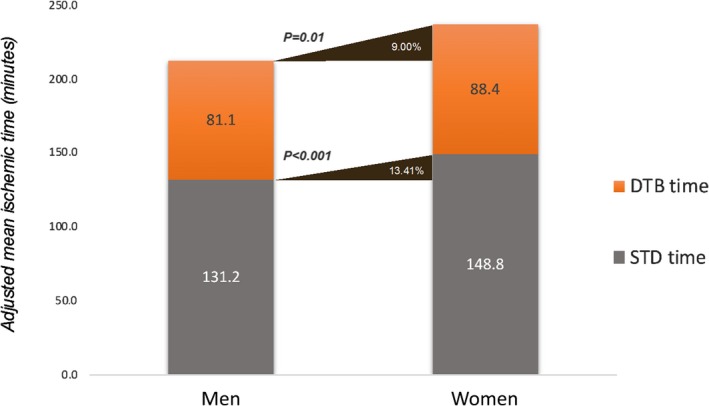
Background Timely revascularization with percutaneous coronary intervention ( PCI ) reduces death following myocardial infarction. We evaluated if a sex gap in symptom-to-door ( STD ), door-to-balloon ( DTB ), and door-to- PCI time persists in contemporary patients, and its impact on mortality. Methods and Results From 2013 to 2016 the Victorian Cardiac Outcomes Registry prospectively recruited 13 451 patients (22.5% female) from 30 centers with ST-segment-elevation myocardial infarction ( STEMI , 47.8%) or non-ST-segment-elevation myocardial infarction (NSTEMI) (52.2%) who underwent PCI . Adjusted log-transformed STD and DTB time in the STEMI cohort and STD and door-to- PCI time in the NSTEMI cohort were analyzed using linear regression. Logistic regression was used to determine independent predictors of 30-day mortality. In STEMI patients, women had longer log- STD time (adjusted geometric mean ratio 1.20, 95% CI 1.12-1.28, P<0.001), log- DTB time (adjusted geometric mean ratio 1.12, 95% CI 1.05-1.20, P=0.001), and 30-day mortality (9.3% versus 6.5%, P=0.005) than men. Womens' adjusted geometric mean STD and DTB times were 28.8 and 7.7 minutes longer, respectively, than were mens' times. Women with NSTEMI had no difference in adjusted STD , door-to- PCI time, or early (<24 hours) versus late revascularization, compared with men. Female sex independently predicted a higher 30-day mortality (odds ratio 1.67, 95% CI 1.11-2.49, P=0.01) in STEMI but not in NSTEMI. Conclusions Women with STEMI have significant delays in presentation and revascularization with a higher 30-day mortality compared with men. The delay in STD time was 4-fold the delay in DTB time. Women with NSTEMI had no delay in presentation or revascularization, with mortality comparable to men. Public awareness campaigns are needed to address women's recognition and early action for STEMI .
Keywords: ST‐segment–elevation myocardial infarction; non–ST‐segment elevation acute coronary syndrome; revascularization.
Figures
Comment in
-
Yentl's Bikini: Sex Differences in STEMI.J Am Heart Assoc. 2019 May 21;8(10):e012873. doi: 10.1161/JAHA.119.012873. J Am Heart Assoc. 2019. PMID: 31092095 Free PMC article.
References
-
- Cannon CP, Gibson CM, Lambrew CT, Shoultz DA, Levy D, French WJ, Gore JM, Weaver WD, Rogers WJ, Tiefenbrunn AJ. Relationship of symptom‐onset‐to‐balloon time and door‐to‐balloon time with mortality in patients undergoing angioplasty for acute myocardial infarction. JAMA. 2000;283:2941–2947. - PubMed
-
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli‐Ducci C, Bueno H, Caforio ALP, Crea F, Goudevenos JA, Halvorsen S, Hindricks G, Kastrati A, Lenzen MJ, Prescott E, Roffi M, Valgimigli M, Varenhorst C, Vranckx P, Widimsky P; ESC Scientific Document Group . 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST‐segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST‐segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39:119–177. - PubMed
-
- Roffi M, Patrono C, Collet JP, Mueller C, Valgimigli M, Andreotti F, Bax JJ, Borger MA, Brotons C, Chew DP, Gencer B, Hasenfuss G, Kjeldsen K, Lancellotti P, Landmesser U, Mehilli J, Mukherjee D, Storey RF, Windecker S; ESC Scientific Document Group . 2015 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST‐segment elevation: Task force for the management of acute coronary syndromes in patients presenting without persistent ST‐segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2016;37:267–315. - PubMed
-
- Jobs A, Mehta SR, Montalescot G, Vicaut E, Van't Hof AWJ, Badings EA, Neumann FJ, Kastrati A, Sciahbasi A, Reuter PG, Lapostolle F, Milosevic A, Stankovic G, Milasinovic D, Vonthein R, Desch S, Thiele H. Optimal timing of an invasive strategy in patients with non‐ST‐elevation acute coronary syndrome: a meta‐analysis of randomised trials. Lancet. 2017;390:737–746. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
