

Prognostic Evaluation of Mortality after Pediatric Resuscitation Assisted by Extracorporeal Life Support
- PMID: 31093456
- PMCID: PMC6517051
- DOI: 10.1055/s-0038-1667012
Prognostic Evaluation of Mortality after Pediatric Resuscitation Assisted by Extracorporeal Life Support
Abstract
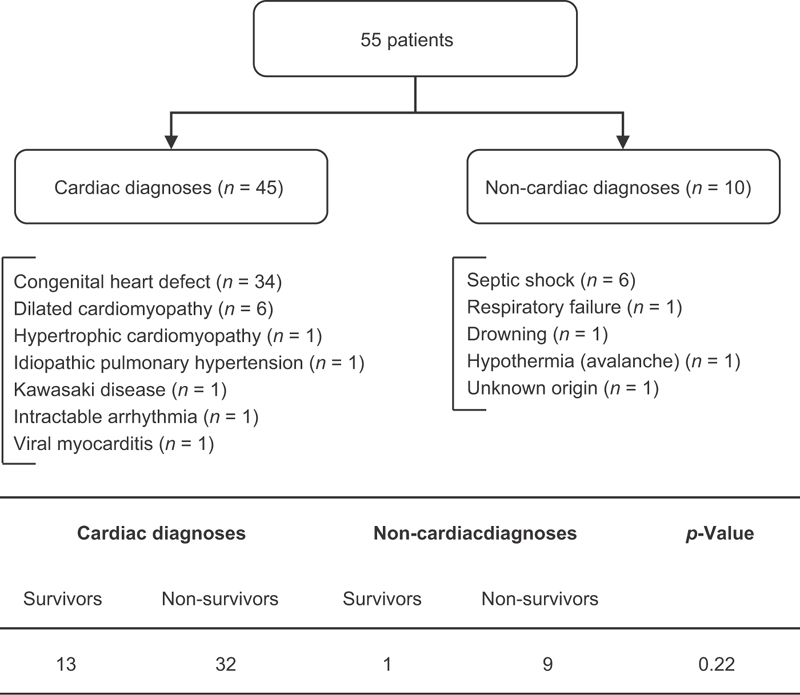
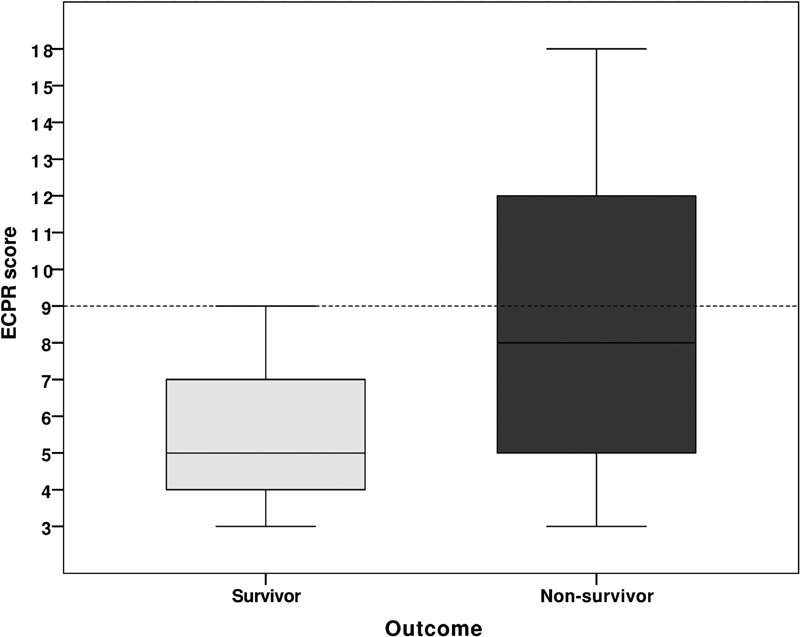
To improve survival rates during cardiopulmonary resuscitation (CPR), some patients are put on extracorporeal life support (ECLS) during active resuscitation (ECPR). Our objective was to assess the clinical outcomes after pediatric ECPR in Switzerland and to determine pre-ECPR prognostic factors for mortality. The present study is a retrospective analysis. The study setting included three pediatric intensive care units in Switzerland that use ECPR. All patients (<16 years old) undergoing ECPR from 2008 to 2016 were included in the study. There were no interventions. Data before ECLS initiation and clinical outcomes were collected. An ECPR score was designed to predict mortality, based on variables significantly different between survivors and non-survivors. Fifty-five patients were included, with a median age of 13.5 months. Eighty percent were cardiac patients. The mortality rate was 75%. Mortality was significantly associated with CPR duration ( p = 0.02), last lactate ( p = 0.05), and last pH ( p = 0.01) before ECLS initiation. Based on these three variables, an ECPR score was designed as follows: CPR duration (in minutes): 1 point if < 40; 2 points if ≥ 40; 3 points if ≥ 60; 6 points if ≥ 105. Lactate (in mmol/L): 1 point if < 8; 2 points if ≥ 8; 3 points if ≥ 14; 6 points if ≥ 18. pH: 1 point if > 7.00; 2 points if ≤ 7.00; 3 points if ≤ 6.85; 6 points if ≤ 6.60. The area under the receiver-operating characteristic curve was 0.74. The positive predictive value of a score ≥ 9 was 94%. In our population, a score based on three variables easily available prior to ECLS initiation had good discrimination and could appropriately predict mortality. This score now needs validation in a larger population.
Keywords: cardiopulmonary resuscitation; children; extracorporeal life support; extracorporeal membrane oxygenation; prognostic factors.
Conflict of interest statement
Figures
References
-
- del Nido P J, Dalton H J, Thompson A E, Siewers R D.Extracorporeal membrane oxygenator rescue in children during cardiac arrest after cardiac surgery Circulation 199286(5, Suppl):II300–II304. - PubMed
-
- Lasa J J, Rogers R S, Localio R et al.Extracorporeal cardiopulmonary resuscitation (E-CPR) during pediatric in-hospital cardiopulmonary arrest is associated with improved survival to discharge: a report from the American Heart Association's Get with the Guidelines-Resuscitation (GWTG-R) Registry. Circulation. 2016;133(02):165–176. - PMC - PubMed
-
- Maconochie I K, de Caen A R, Aickin R et al.Part 6: Pediatric basic life support and pediatric advanced life support: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation. 2015;95:e147–e168. - PubMed
-
- Joffe A R, Lequier L, Robertson C M. Pediatric outcomes after extracorporeal membrane oxygenation for cardiac disease and for cardiac arrest: a review. ASAIO J. 2012;58(04):297–310. - PubMed
LinkOut - more resources
Full Text Sources
