

Physical Activity, All-Cause and Cardiovascular Mortality, and Cardiovascular Disease
- PMID: 31095084
- PMCID: PMC6527136
- DOI: 10.1249/MSS.0000000000001939
Physical Activity, All-Cause and Cardiovascular Mortality, and Cardiovascular Disease
Abstract
Purpose: Conduct a systematic umbrella review to evaluate the relationship of physical activity (PA) with all-cause mortality, cardiovascular mortality, and incident cardiovascular disease (CVD); to evaluate the shape of the dose-response relationships; and to evaluate these relationships relative to the 2008 Physical Activity Guidelines Advisory Committee Report.
Methods: Primary search encompassing 2006 to March, 2018 for existing systematic reviews, meta-analyses, and pooled analyses reporting on these relationships. Graded the strength of evidence using a matrix developed for the Physical Activity Guidelines Advisory Committee.
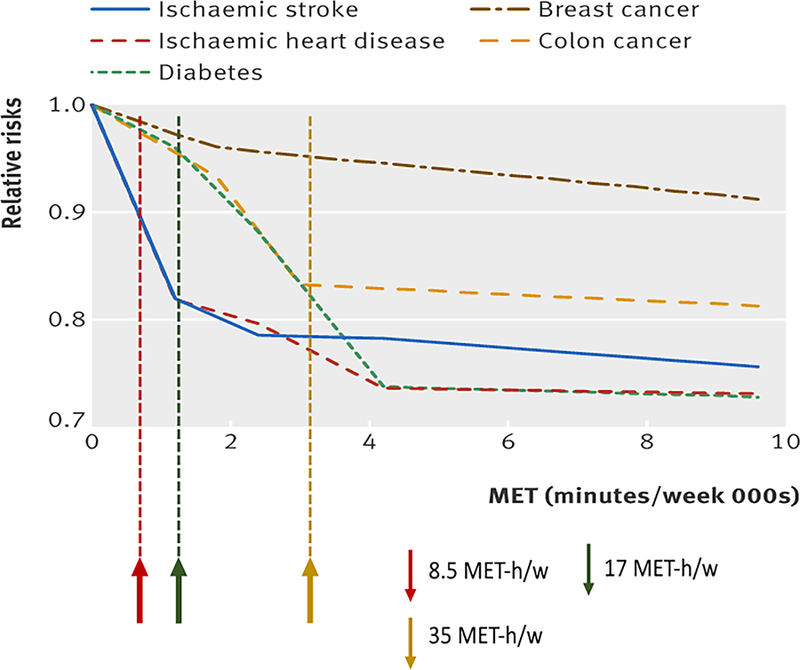
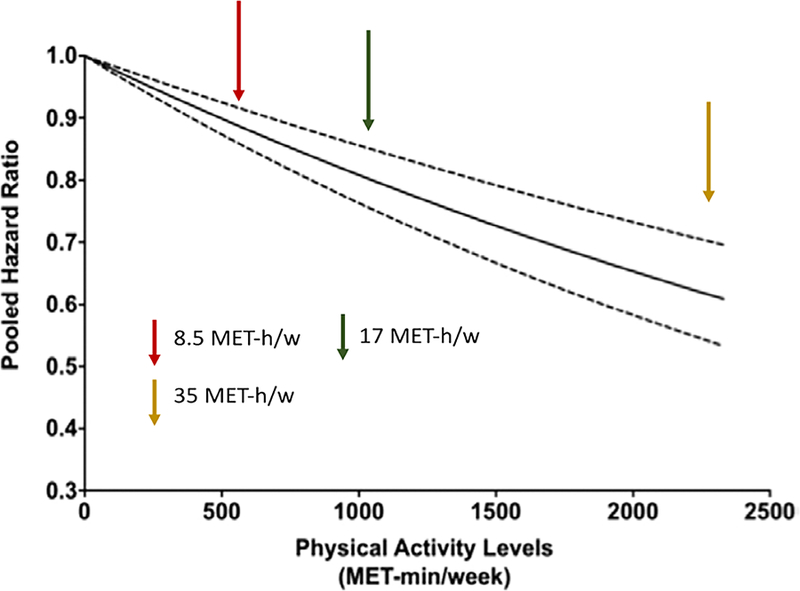
Results: The association of self-reported moderate-to-vigorous physical activity (MVPA) on all-cause mortality, CVD mortality, and atherosclerotic CVD-including incident coronary heart disease, ischemic stroke and heart failure-are very similar. Increasing MVPA to guidelines amounts in the inactive US population has the potential to have an important and substantial positive impact on these outcomes in the adult population. The following points are clear: the associations of PA with beneficial health outcomes begin when adopting very modest (one-third of guidelines) amounts; any MVPA is better than none; meeting the 2008 PA guidelines reduces mortality and CVD risk to about 75% of the maximal benefit obtained by physical activity alone; PA amounts beyond guidelines recommendations amount reduces risk even more, but greater amounts of PA are required to obtain smaller health benefits; and there is no evidence of excess risk over the maximal effect observed at about three to five times the amounts associated with current guidelines. When PA is quantified in terms of energy expenditure (MET·h·wk), these relationships hold for walking, running, and biking.
Conclusions: To avoid the risks associated with premature mortality and the development of ischemic heart disease, ischemic stroke, and all-cause heart failure, all adults should strive to reach the 2008 Physical Activity Guidelines for Americans.
Conflict of interest statement
Conflicts of Interest and Source of Funding
The results of this study are presented clearly, honestly, and without fabrication, falsification, or inappropriate manipulation. The Committee’s work was supported by the U.S. Department of Health and Human Services (HHS). Committee members were reimbursed for travel and per diem expenses for the five public meetings; Committee members volunteered their time. The authors report no other potential conflicts of interest.
Figures
References
-
- Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Scientific Report Washington, DC: U.S. Department of Health and Human Services; 2008.
-
- Physical Activity Guidelines for Americans In: DHHS, editor. Washington, DC: U.S. Department of Health and Human Services; 2008.
-
- Physical Activity Guidelines Advisory Committee 2018. 2018 Physical Activity Guidelines Advisory Committee Scientific Report Washington, DC: U.S. Department of Health and Human Services; 2018.
-
- Torres A, Tennant B, Ribeiro-Lucas I, Vaux-Bjerke A, Piercy K, Bloodgood B. Umbrella and systematic review methodology to support the 2018 Physical Activity Guidelines Advisory Committee. J Phys Act Health 2018;1–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
