

Visual Acuity and Ophthalmic Outcomes in the Year After Cataract Surgery Among Children Younger Than 13 Years
- PMID: 31095258
- PMCID: PMC6537788
- DOI: 10.1001/jamaophthalmol.2019.1220
Visual Acuity and Ophthalmic Outcomes in the Year After Cataract Surgery Among Children Younger Than 13 Years
Abstract
Importance: Cataract is an important cause of visual impairment in children. Outcomes reported from a large clinical disease-specific registry can provide real-world estimates of visual outcomes and rates of adverse events in clinical practice.
Objective: To describe visual acuity and refractive error outcomes, as well as rates of amblyopia, glaucoma, and additional eye surgery, during the first year after lensectomy in children.
Design, setting, and participants: A prospective observational study was conducted from June 18, 2012, to July 8, 2015, at 61 pediatric eye care practices among 880 children younger than 13 years at the time of lensectomy in at least 1 eye with follow-up within 15 months after surgery. Statistical analysis was performed from December 12, 2016, to December 14, 2018.
Exposures: Lensectomy with or without implantation of an intraocular lens.
Main outcomes and measures: Visual acuity as well as rates of amblyopia, glaucoma, suspected glaucoma, and other intraocular surgery.
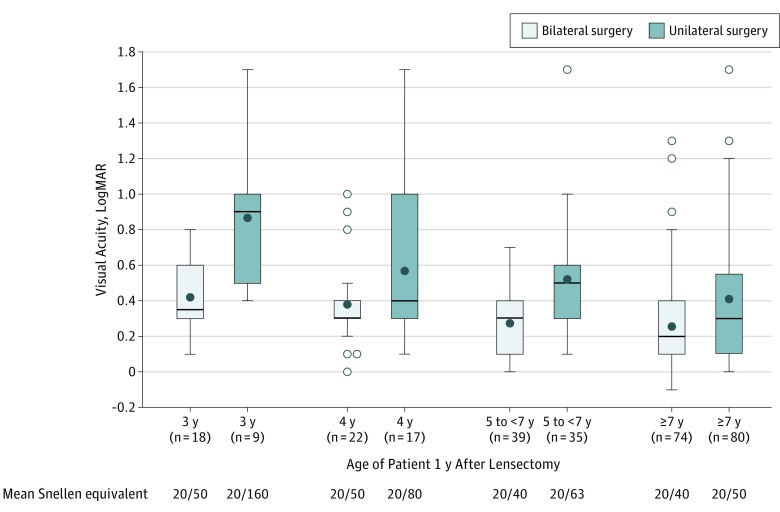
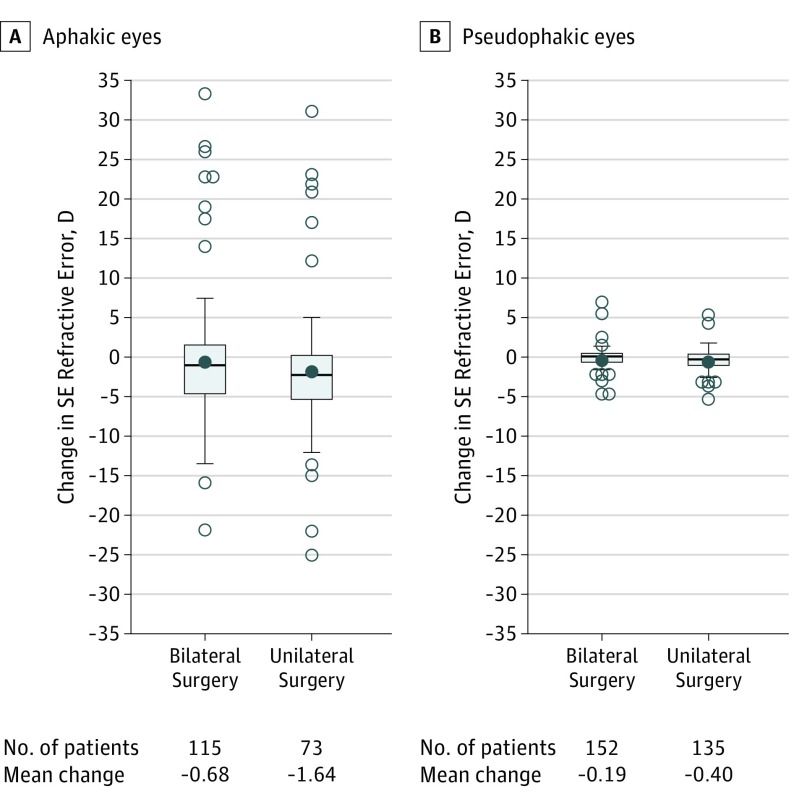
Results: Among the 880 children (432 girls and 448 boys; mean [SD] age at annual follow-up, 4.9 [3.8] years) in the study, lens surgery was bilateral in 362 (41.1%; 95% CI, 37.9%-44.4%) children and unilateral in 518 (58.9%; 95% CI, 55.6%-62.1%). An intraocular lens was implanted in 654 of 1132 eyes (60.2%; 95% CI, 57.0%-63.4% [proportions reported for eye-level outcomes account for the potential correlation induced by enrolling both eyes of some individuals; for participants who received bilateral surgery, these numbers will differ from the quotient of the number of cases divided by the total sample size]). Amblyopia was identified in 449 children (51.0%; 95% CI, 47.7%-54.3%). In children age 3 years or older, mean visual acuity was 0.30 logMAR (about 20/40) in 153 bilateral pseudophakic eyes, 0.49 logMAR (about 20/63) in 141 unilateral pseudophakic eyes, 0.47 logMAR (about 20/63) in 21 bilateral aphakic eyes, and 0.61 logMAR (about 20/80) in 17 unilateral aphakic eyes. Mean visual acuity improved with older age at surgery in eyes with bilateral pseudophakia by 0.2 logMAR line (99% CI, 0.02-0.4; P = .005) and by 0.3 logMAR line (99% CI, 0.04-0.60; P = .004) in eyes with unilateral pseudophakia. A new diagnosis of glaucoma or suspected glaucoma was made in 67 of 1064 eyes that did not have glaucoma prior to lensectomy (5.9%; 95% CI, 4.6%-7.7%); 36 of 273 eyes with bilateral aphakia (13.2%; 95% CI, 9.0%-19.0%), 5 of 308 eyes with bilateral pseudophakia (1.5%; 95% CI, 0.6%-4.2%), 14 of 178 eyes with unilateral aphakia (7.9%; 95% CI, 4.7%-12.8%), and 12 of 305 eyes with unilateral pseudophakia (3.9%; 95% CI, 2.2%-6.8%). Additional intraocular surgery, most commonly vitrectomy or membranectomy to clear the visual axis, was performed in 189 of 1132 eyes (17.0%; 95% CI, 14.8%-19.6%).
Conclusions and relevance: Amblyopia was frequently observed during the first year after lensectomy in this cohort of children younger than 13 years. For children age 2 years or older at surgery visual acuity was typically less than normal for age and was worse with unilateral cataract. Management of visual axis obscuration was the most common complication requiring surgical intervention during the first year after surgery.
Conflict of interest statement
Figures
References
-
- Drover JR, Felius J, Cheng CS, Morale SE, Wyatt L, Birch EE. Normative pediatric visual acuity using single surrounded HOTV optotypes on the Electronic Visual Acuity Tester following the Amblyopia Treatment Study protocol. J AAPOS. 2008;12(2):145-149. doi: 10.1016/j.jaapos.2007.08.014 - DOI - PMC - PubMed
-
- Lambert SR, Fernandes A, Drews-Botsch C, Tigges M. Pseudophakia retards axial elongation in neonatal monkey eyes. Invest Ophthalmol Vis Sci. 1996;37(2):451-458. - PubMed
