

Resistance diagnostics as a public health tool to combat antibiotic resistance: A model-based evaluation
- PMID: 31095567
- PMCID: PMC6522007
- DOI: 10.1371/journal.pbio.3000250
Resistance diagnostics as a public health tool to combat antibiotic resistance: A model-based evaluation
Abstract
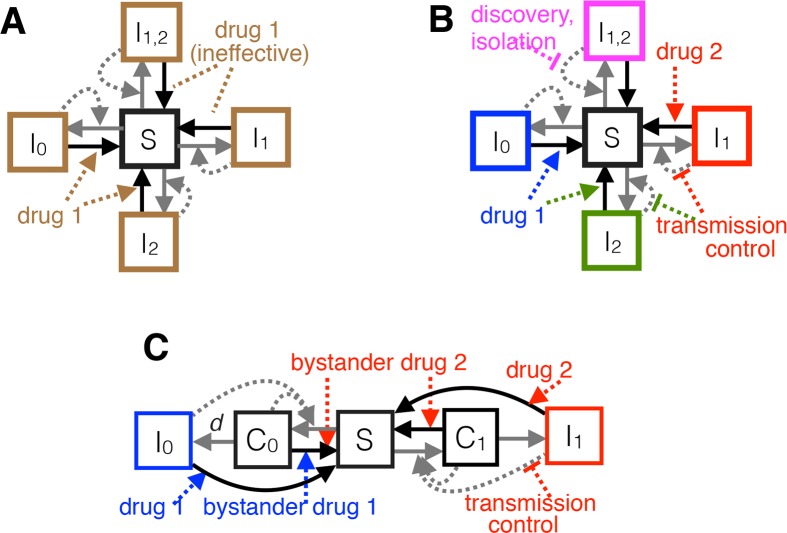
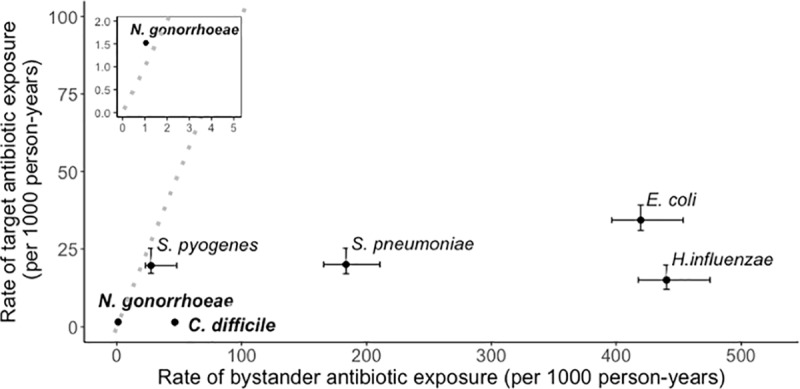
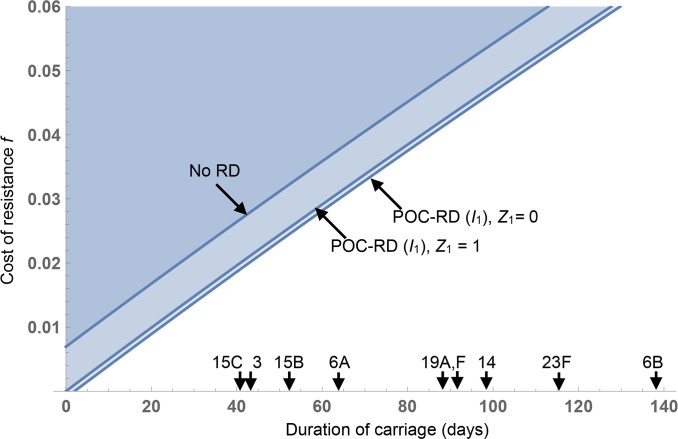
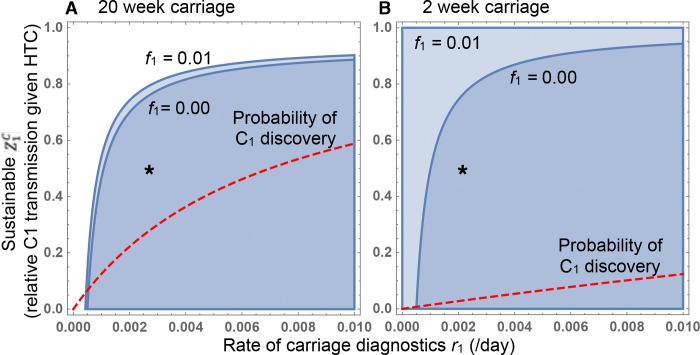
Rapid point-of-care resistance diagnostics (POC-RD) are a key tool in the fight against antibiotic resistance. By tailoring drug choice to infection genotype, doctors can improve treatment efficacy while limiting costs of inappropriate antibiotic prescription. Here, we combine epidemiological theory and data to assess the potential of resistance diagnostics (RD) innovations in a public health context, as a means to limit or even reverse selection for antibiotic resistance. POC-RD can be used to impose a nonbiological fitness cost on resistant strains by enabling diagnostic-informed treatment and targeted interventions that reduce resistant strains' opportunities for transmission. We assess this diagnostic-imposed fitness cost in the context of a spectrum of bacterial population biologies and find that POC-RD have a greater potential against obligate pathogens than opportunistic pathogens already subject to selection under "bystander" antibiotic exposure during asymptomatic carriage (e.g., the pneumococcus). We close by generalizing the notion of RD-informed strategies to incorporate carriage surveillance information and illustrate that coupling transmission-control interventions to the discovery of resistant strains in carriage can potentially select against resistance in a broad range of opportunistic pathogens.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Centers for Disease Control and Prevention. Antibiotic resistance threats in the United States, 2013. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 2013.
-
- Center for Disease Dynamics Economics & Policy. The state of the world’s antibiotics 2015. Washington, D.C.: The Center; 2015.
-
- World Health Organization. Antimicrobial resistance Fact Sheet 194 [Internet]. Geneva: The Organization; 2014. April Available from: http://www.wpro.who.int/mediacentre/releases/2014/AMR_factsheet_FINAL.pdf. [cited 2019 Apr 3].
-
- European Centre for Disease Prevention and Control. Antimicrobial resistance surveillance in Europe 2014. Solna (Sweden): The Centre; 2015.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
