

The role of evidence-based algorithms for rotational thromboelastometry-guided bleeding management
- PMID: 31096732
- PMCID: PMC6676023
- DOI: 10.4097/kja.19169
The role of evidence-based algorithms for rotational thromboelastometry-guided bleeding management
Abstract
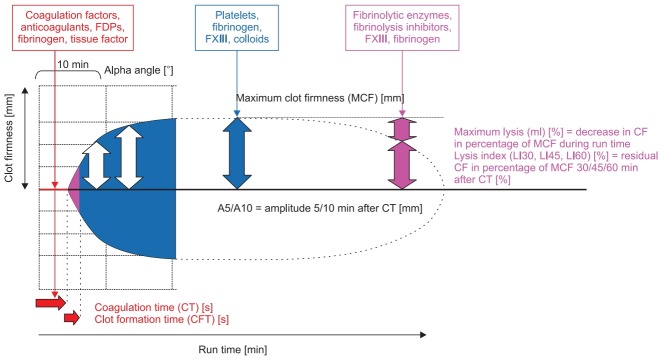
Rotational thromboelastometry (ROTEM) is a point-of-care viscoelastic method and enables to assess viscoelastic profiles of whole blood in various clinical settings. ROTEM-guided bleeding management has become an essential part of patient blood management (PBM) which is an important concept in improving patient safety. Here, ROTEM testing and hemostatic interventions should be linked by evidence-based, setting-specific algorithms adapted to the specific patient population of the hospitals and the local availability of hemostatic interventions. Accordingly, ROTEM-guided algorithms implement the concept of personalized or precision medicine in perioperative bleeding management ('theranostic' approach). ROTEM-guided PBM has been shown to be effective in reducing bleeding, transfusion requirements, complication rates, and health care costs. Accordingly, several randomized-controlled trials, meta-analyses, and health technology assessments provided evidence that using ROTEM-guided algorithms in bleeding patients resulted in improved patient's safety and outcomes including perioperative morbidity and mortality. However, the implementation of ROTEM in the PBM concept requires adequate technical and interpretation training, education and logistics, as well as interdisciplinary communication and collaboration.
Keywords: Algorithms; Bleeding management; Health care costs; Impedance aggregometry; Patient blood management; Thromboelastometry.
Conflict of interest statement
Klaus Görlinger is working as the Medical Director of Tem Innovations since July 2012. Daniel Dirkmann, Fuat Saner and Marc Maegele are members of the scientific advisory committee of Instrumentation Laboratory and received travel expense refunds and speakers fees from Tem Innovations, Instrumentation Laboratory/Werfen, and CSL Behring. Antonio Pérez-Ferrer, Angelo Augusto Pérez Calatayud and Tae-Yop Kim reported no potential conflict of interest relevant to this article.
Figures
References
-
- Zacharowski K, Spahn DR. Patient blood management equals patient safety. Best Pract Res Clin Anaesthesiol. 2016;30:159–69. - PubMed
-
- Bochicchio GV, Napolitano L, Joshi M, Bochicchio K, Meyer W, Scalea TM. Outcome analysis of blood product transfusion in trauma patients: a prospective, risk-adjusted study. World J Surg. 2008;32:2185–9. - PubMed
-
- Ranucci M, Baryshnikova E, Castelvecchio S, Pelissero G. Major bleeding, transfusions, and anemia: the deadly triad of cardiac surgery. Ann Thorac Surg. 2013;96:478–85. - PubMed
-
- Turan A, Yang D, Bonilla A, Shiba A, Sessler DI, Saager L, et al. Morbidity and mortality after massive transfusion in patients undergoing non-cardiac surgery. Can J Anaesth. 2013;60:761–70. - PubMed
-
- Ruseckaite R, McQuilten ZK, Oldroyd JC, Richter TH, Cameron PA, Isbister JP, et al. Descriptive characteristics and in-hospital mortality of critically bleeding patients requiring massive transfusion: results from the Australian and New Zealand Massive Transfusion Registry. Vox Sang. 2017;112:240–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
