

Risk assessment models for potential use in the emergency department have lower predictive ability in older patients compared to the middle-aged for short-term mortality - a retrospective cohort study
- PMID: 31096925
- PMCID: PMC6521424
- DOI: 10.1186/s12877-019-1154-7
Risk assessment models for potential use in the emergency department have lower predictive ability in older patients compared to the middle-aged for short-term mortality - a retrospective cohort study
Abstract
Background: Older patients is a complex group at increased risk of adverse outcomes compared to younger patients, which should be considered in the risk assessment performed in emergency departments. We evaluated whether the predictive ability of different risk assessment models for acutely admitted patients is affected by age.
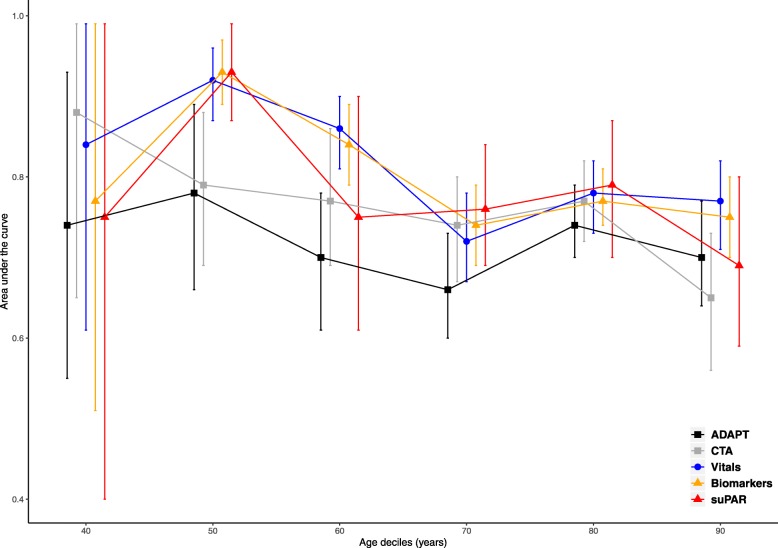
Methods: Cohort study of middle-aged and older patients. We investigated the accuracy in discriminating between survivors and non-survivors within 7 days of different risk assessment models; a traditional triage algorithm, a triage algorithm with clinical assessment, vital signs, routine biomarkers, and the prognostic biomarker soluble urokinase plasminogen activator receptor (suPAR).
Results: The cohort included 22,653 (53.2%) middle-aged patients (age 40-69 years), and 19,889 (46.8%) older patients (aged 70+ years). Death within 7 days occurred in 139 patients (0.6%) in middle-aged patients and 596 (3.0%) of the older patients. The models based on vital signs and routine biomarkers had the highest area under the curve (AUC), and both were significantly better at discriminating 7-day mortality in middle-aged patients compared to older patients; AUC (95% CI): 0.88 (0.84-0.91), 0.75 (0.72-0.78), P < 0.01, and 0.86 (0.82-0.90), 0.76 (0.73-0.78), P < 0.001. In a subgroup of the total cohort (6.400 patients, 15.0%), the suPAR level was available. suPAR had the highest AUC of all individual predictors with no significant difference between the age groups, but further research in this biomarker is required before it can be used.
Conclusion: The predictive value was lower in older patients compared to middle-aged patients for all investigated models. Vital signs or routine biomarkers constituted the best models for predicting 7-day mortality and were better than the traditional triage model. Hence, the current risk assessment for short-term mortality can be strengthened, but modifications for age should be considered when constructing new risk assessment models in the emergency department.
Keywords: Emergency department; Older patients; Risk assessment; Triage.
Conflict of interest statement
Ethics approval and consent to participate
The TRIAGE studies were approved by Danish Patient Safety Authority instead of patient consent, in accordance with Danish legislation. All processing of personal data followed national guidelines and was approved by the Danish Data Protection Agency. Both TRIAGE studies were presented to the regional independent ethics committee, who decided that no consent were required in accordance with Danish law.
Consent for publication
Not applicable.
Competing interests
MS and LJHR have received funding for travel from ViroGates A/S. JE-O is named as an inventor in patents for the use of suPAR as a prognostic biomarker. The patents are owned by Copenhagen University Hospital, Amager and Hvidovre, Denmark, and are licensed to ViroGates A/S. JE-O is a co-founder, shareholder, and CSO of ViroGates A/S. The remaining authors have no conflicts of interest to declare.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
