

Association of cardiovascular magnetic resonance-derived circumferential strain parameters with the risk of ventricular arrhythmia and all-cause mortality in patients with prior myocardial infarction and primary prevention implantable cardioverter defibrillator
- PMID: 31096987
- PMCID: PMC6521513
- DOI: 10.1186/s12968-019-0536-5
Association of cardiovascular magnetic resonance-derived circumferential strain parameters with the risk of ventricular arrhythmia and all-cause mortality in patients with prior myocardial infarction and primary prevention implantable cardioverter defibrillator
Abstract
Background: Impaired left ventricular (LV) contraction and relaxation may further promote adverse remodeling and may increase the risk of ventricular arrhythmia (VA) in ischemic cardiomyopathy. We aimed to examine the association of cardiovascular magnetic resonance (CMR)-derived circumferential strain parameters for LV regional systolic function, LV diastolic function and mechanical dispersion with the risk of VA in patients with prior myocardial infarction and primary prevention implantable cardioverter defibrillator (ICD).
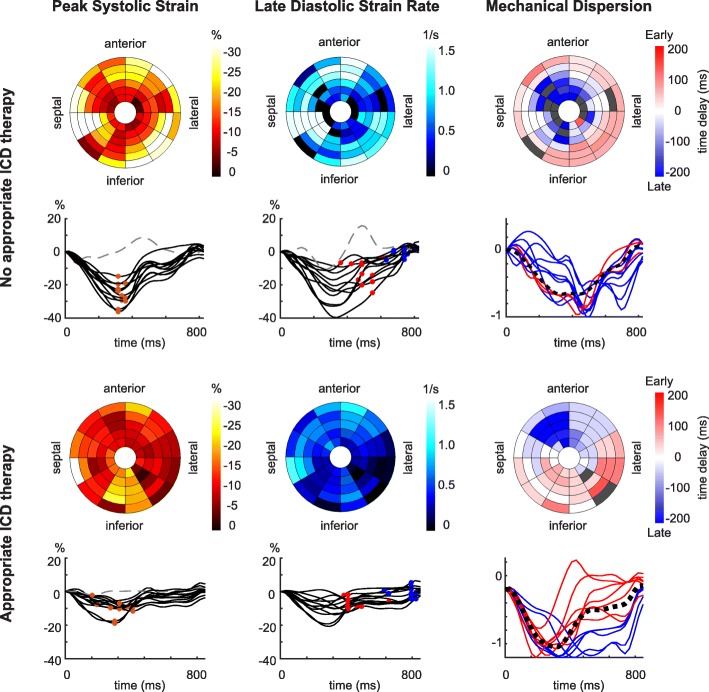
Methods: Patients with an ischemic cardiomyopathy who underwent CMR prior to primary prevention ICD implantation, were retrospectively identified. LV segmental circumferential strain curves were extracted from short-axis cine CMR. For LV regional strain analysis, the extent of moderately and severely impaired strain (percentage of LV segments with strain between - 10% and - 5% and > - 5%, respectively) were calculated. LV diastolic function was quantified by the early and late diastolic strain rate. Mechanical dispersion was defined as the standard deviation in delay time between each strain curve and the patient-specific reference curve. Cox proportional hazard ratios (HR) (95%CI) were calculated to assess the association between LV strain parameters and appropriate ICD therapy.
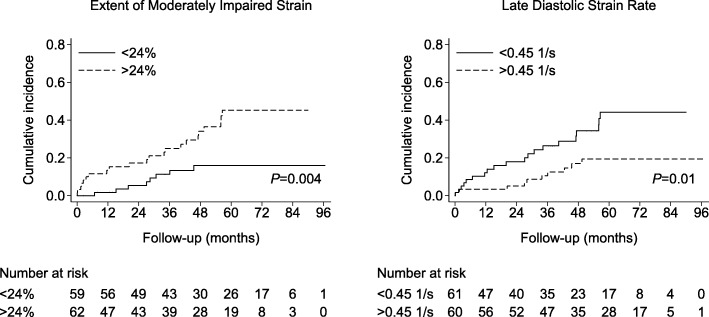
Results: A total of 121 patients (63 ± 11 years, 84% men, LV ejection fraction (LVEF) 27 ± 9%) were included. During a median (interquartile range) follow-up of 47 (27;69) months, 30 (25%) patients received appropriate ICD therapy. The late diastolic strain rate (HR 1.1 (1.0;1.2) per - 0.25 1/s, P = 0.043) and the extent of moderately impaired strain (HR 1.5 (1.0;2.2) per + 10%, P = 0.048) but not the extent of severely impaired strain (HR 0.9 (0.6;1.4) per + 10%, P = 0.685) were associated with appropriate ICD therapy, independent of LVEF, late gadolinium enhancement (LGE) scar border size and acute revascularization. Mechanical dispersion was not related to appropriate ICD therapy (HR 1.1 (0.8;1.6) per + 25 ms, P = 0.464).
Conclusions: In an ischemic cardiomyopathy population referred for primary prevention ICD implantation, the extent of moderately impaired strain and late diastolic strain rate were associated with the risk of appropriate ICD therapy, independent of LVEF, scar border size and acute revascularization. These findings suggest that disturbed LV contraction and relaxation may contribute to an increased risk of VA after myocardial infarction.
Keywords: Circumferential strain; Ischemic cardiomyopathy; Magnetic resonance; Ventricular arrhythmia.
Conflict of interest statement
Ethics approval and consent to participate
Informed consent in this retrospective study was waived by the local institutional review board (Leiden University Medical Center, the Netherlands).
Consent for publication
Not applicable.
Competing interests
The Department of Cardiology (Leiden University Medical Center, Leiden, The Netherlands) receives unrestricted research grants from Edwards Lifesciences, Medtronic, Biotronik and Boston Scientific.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Cardiovascular Magnetic Resonance to Predict Appropriate Implantable Cardioverter Defibrillator Therapy in Ischemic and Nonischemic Cardiomyopathy Patients Using Late Gadolinium Enhancement Border Zone: Comparison of Four Analysis Methods.Circ Cardiovasc Imaging. 2017 Sep;10(9):e006105. doi: 10.1161/CIRCIMAGING.116.006105. Circ Cardiovasc Imaging. 2017. PMID: 28838961 Free PMC article.
-
Left Ventricular Entropy Is a Novel Predictor of Arrhythmic Events in Patients With Dilated Cardiomyopathy Receiving Defibrillators for Primary Prevention.JACC Cardiovasc Imaging. 2019 Jul;12(7 Pt 1):1177-1184. doi: 10.1016/j.jcmg.2018.07.003. Epub 2018 Aug 15. JACC Cardiovasc Imaging. 2019. PMID: 30121262
-
Infarct tissue characterization in implantable cardioverter-defibrillator recipients for primary versus secondary prevention following myocardial infarction: a study with contrast-enhancement cardiovascular magnetic resonance imaging.Int J Cardiovasc Imaging. 2013 Jan;29(1):169-76. doi: 10.1007/s10554-012-0077-6. Epub 2012 Jun 9. Int J Cardiovasc Imaging. 2013. PMID: 22684301 Free PMC article.
-
When to consider an implantable cardioverter defibrillator following myocardial infarction?Heart. 2015 Dec;101(24):1996-2000. doi: 10.1136/heartjnl-2015-307788. Epub 2015 Nov 2. Heart. 2015. PMID: 26526420 Review.
-
Myocardial Fibrosis Assessment by LGE Is a Powerful Predictor of Ventricular Tachyarrhythmias in Ischemic and Nonischemic LV Dysfunction: A Meta-Analysis.JACC Cardiovasc Imaging. 2016 Sep;9(9):1046-1055. doi: 10.1016/j.jcmg.2016.01.033. Epub 2016 Jul 20. JACC Cardiovasc Imaging. 2016. PMID: 27450871 Review.
Cited by
-
MRI Assessment of Myocardial Deformation for Risk Stratification of Major Arrhythmic Events in Patients With Non-Ischemic Cardiomyopathy Eligible for Primary Prevention Implantable Cardioverter Defibrillators.J Magn Reson Imaging. 2024 Nov;60(5):1976-1986. doi: 10.1002/jmri.29238. Epub 2024 Jan 19. J Magn Reson Imaging. 2024. PMID: 38240166
-
Atrial and Ventricular Strain Imaging Using CMR in the Prediction of Ventricular Arrhythmia in Patients with Myocarditis.J Clin Med. 2024 Jan 23;13(3):662. doi: 10.3390/jcm13030662. J Clin Med. 2024. PMID: 38337355 Free PMC article.
-
Quantification of Myocardial Deformation Applying CMR-Feature-Tracking-All About the Left Ventricle?Curr Heart Fail Rep. 2021 Aug;18(4):225-239. doi: 10.1007/s11897-021-00515-0. Epub 2021 May 1. Curr Heart Fail Rep. 2021. PMID: 33931818 Free PMC article. Review.
-
Cardiac magnetic resonance-derived mitral annular plane systolic excursion: a robust indicator for risk stratification after myocardial infarction.Int J Cardiovasc Imaging. 2024 Apr;40(4):897-906. doi: 10.1007/s10554-024-03058-2. Epub 2024 Feb 24. Int J Cardiovasc Imaging. 2024. PMID: 38400864
-
Myocardial strain assessment using cardiovascular magnetic resonance imaging in recipients of implantable cardioverter defibrillators.J Cardiovasc Magn Reson. 2021 Oct 21;23(1):115. doi: 10.1186/s12968-021-00806-4. J Cardiovasc Magn Reson. 2021. PMID: 34670574 Free PMC article.
References
-
- Brignole M, Auricchio A, Baron-Esquivias G, Bordachar P, Boriani G, Breithardt OA, et al. 2013 ESC guidelines on cardiac pacing and cardiac resynchronization therapy: the task force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA) Eur Heart J. 2013;34(29):2281–2329. - PubMed
-
- Moss AJ, Greenberg H, Case RB, Zareba W, Hall WJ, Brown MW, et al. Long-term clinical course of patients after termination of ventricular tachyarrhythmia by an implanted defibrillator. Circulation. 2004;110(25):3760–3765. - PubMed
-
- St John Sutton M, Lee D, Rouleau JL, Goldman S, Plappert T, Braunwald E, et al. Left ventricular remodeling and ventricular arrhythmias after myocardial infarction. Circulation. 2003;107(20):2577–2582. - PubMed
-
- Gaudron P, Kugler I, Hu K, Bauer W, Eilles C, Ertl G. Time course of cardiac structural, functional and electrical changes in asymptomatic patients after myocardial infarction: their inter-relation and prognostic impact. J Am Coll Cardiol. 2001;38(1):33–40. - PubMed
-
- D'Elia N, D'Hooge J, Marwick TH. Association between myocardial mechanics and ischemic LV remodeling. JACC Cardiovasc Imaging. 2015;8(12):1430–1443. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
