

Insights on multimorbidity and associated health service use and costs from three population-based studies of older adults in Ontario with diabetes, dementia and stroke
- PMID: 31096989
- PMCID: PMC6524233
- DOI: 10.1186/s12913-019-4149-3
Insights on multimorbidity and associated health service use and costs from three population-based studies of older adults in Ontario with diabetes, dementia and stroke
Abstract
Background: Most studies that examine comorbidity and its impact on health service utilization focus on a single index-condition and are published in disease-specific journals, which limit opportunities to identify patterns across conditions/disciplines. These comparisons are further complicated by the impact of using different study designs, multimorbidity definitions and data sources. The aim of this paper is to share insights on multimorbidity and associated health services use and costs by reflecting on the common patterns across 3 parallel studies in distinct disease cohorts (diabetes, dementia, and stroke) that used the same study design and were conducted in the same health jurisdiction over the same time period.
Methods: We present findings that lend to broader Insights regarding multimorbidity based on the relationship between comorbidity and health service use and costs seen across three distinct disease cohorts. These cohorts were originally created using multiple linked administrative databases to identify community-dwelling residents of Ontario, Canada with one of diabetes, dementia, or stroke in 2008 and each was followed for health service use and associated costs.
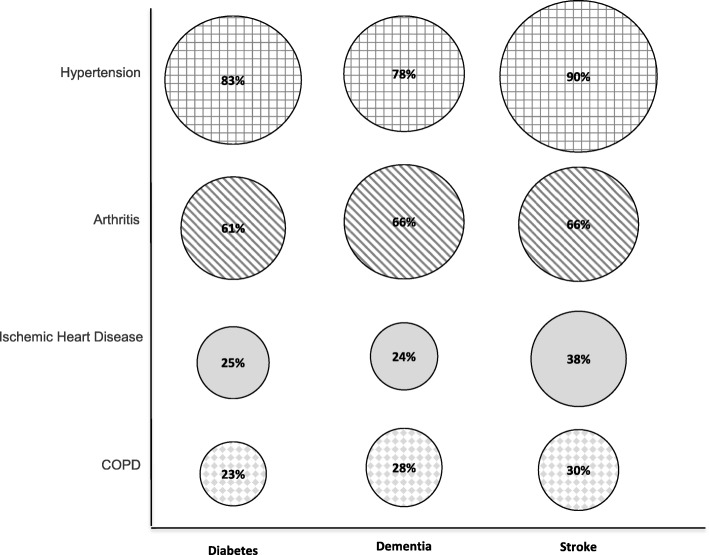
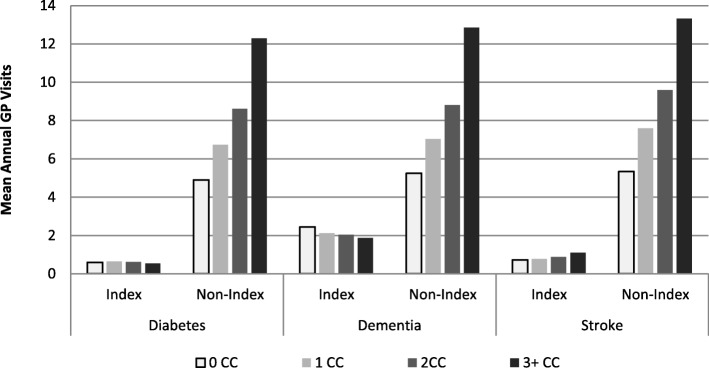
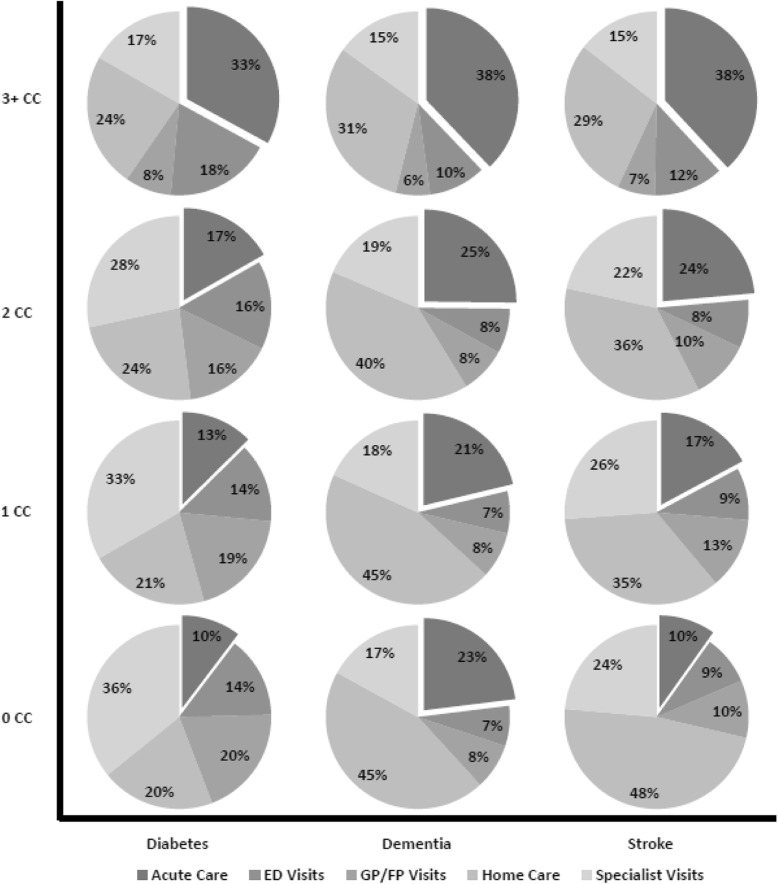
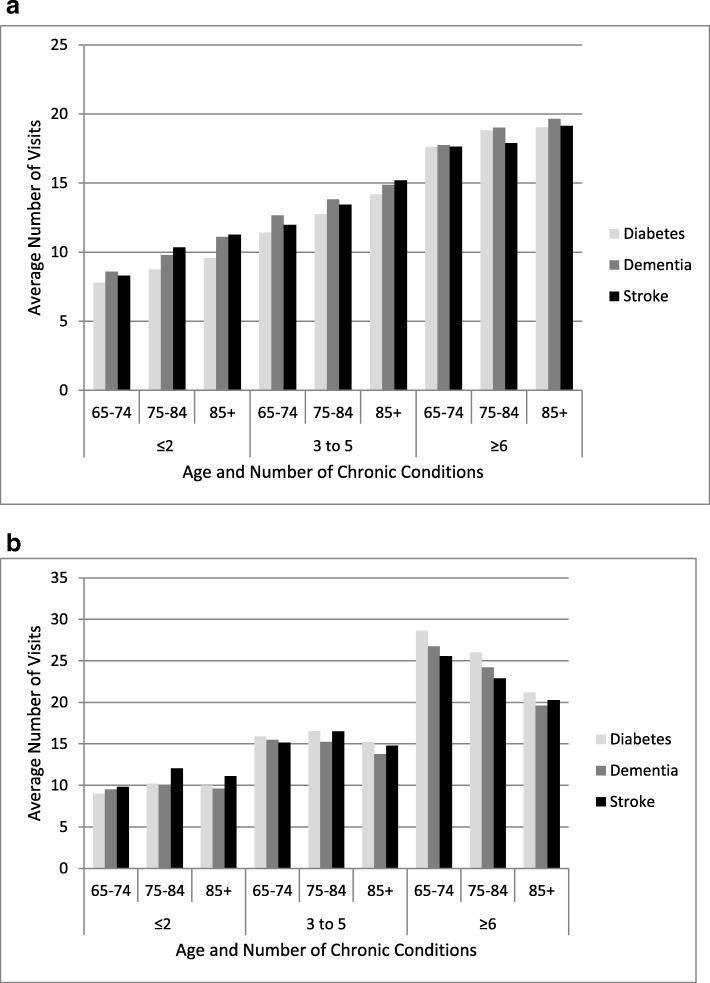
Results: We identified 376,434 indviduals wtih diabetes, 95,399 wtih dementia, and 29,671 with stroke. Four broad insights were identified from considering the similarity in comorbidity, utilization and cost patterns across the three cohorts: 1) the most prevalent comorbidity types were hypertension and arthritis, which accounted for over 75% of comorbidity in each cohort; 2) overall utilization increased consistently with the number of comorbidities, with the vast majority of services attributed to comorbidity rather than the index conditions; 3) the biggest driver of costs for those with lower levels of comorbidity was community-based care, e.g., home care, GP visits, but at higher levels of comorbidity the driver was acute care services; 4) service-specific comorbidity and age patterns were consistent across the three cohorts.
Conclusions: Despite the differences in population demographics and prevalence of the three index conditions, there are common patterns with respect to comorbidity, utilization, and costs. These common patterns may illustrate underlying needs of people with multimorbidity that are often obscured in literature that is still single disease-focused.
Keywords: Community-living older adults; Comorbidity; Health service costs; Health service utilization; Multimorbidity.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Boyd CM, Fortin M. Future of multimorbidity research: how should understanding of multimorbidity inform health system design? Public Health Rev. 2010;32:451–474. doi: 10.1007/BF03391611. - DOI
-
- American Geriatrics Society Expert Panel on the Care of Older Adults with Multimorbidity Guiding principles for the care of older adults with multimorbidity: an approach for clinicians: American Geriatrics Society expert panel on the Care of Older Adults with multimorbidity. J Am Geriatr Soc. 2012;60:E1–E25. doi: 10.1111/j.1532-5415.2012.04188.x. - DOI - PMC - PubMed
-
- Farmer C, Fenu E, O'Flynn N, Guthrie B. Clinical assessment and management of multimorbidity: summary of NICE guidance. BMJ. 2016;354:i4843. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
