

Pacemaker Implantation After Mitral Valve Surgery With Atrial Fibrillation Ablation
- PMID: 31097163
- PMCID: PMC6602091
- DOI: 10.1016/j.jacc.2019.02.062
Pacemaker Implantation After Mitral Valve Surgery With Atrial Fibrillation Ablation
Abstract
Background: The incidence of permanent pacemaker (PPM) implantation is higher following mitral valve surgery (MVS) with ablation for atrial fibrillation (AF) compared with MVS alone.
Objectives: This study identified risk factors and outcomes associated with PPM implantation in a randomized trial that evaluated ablation for AF in patients who underwent MVS.
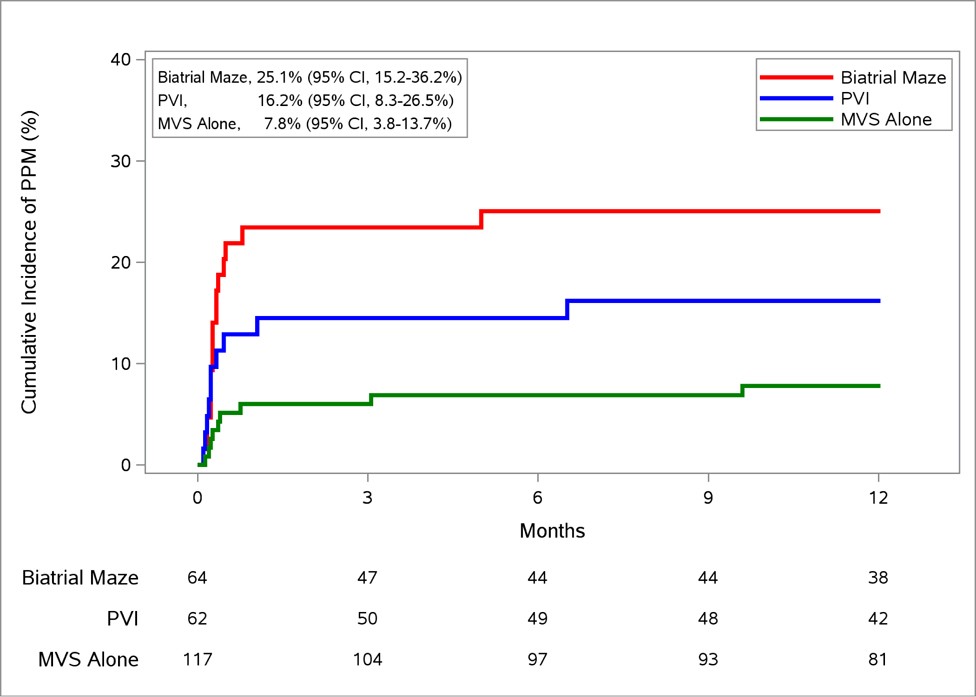
Methods: A total of 243 patients with AF and without previous PPM placement were randomly assigned to MVS alone (n = 117) or MVS + ablation (n = 126). Patients in the ablation group were further randomized to pulmonary vein isolation (PVI) (n = 62) or the biatrial maze procedure (n = 64). Using competing risk models, this study examined the association among PPM and baseline and operative risk factors, and the effect of PPM on time to discharge, readmissions, and 1-year mortality.
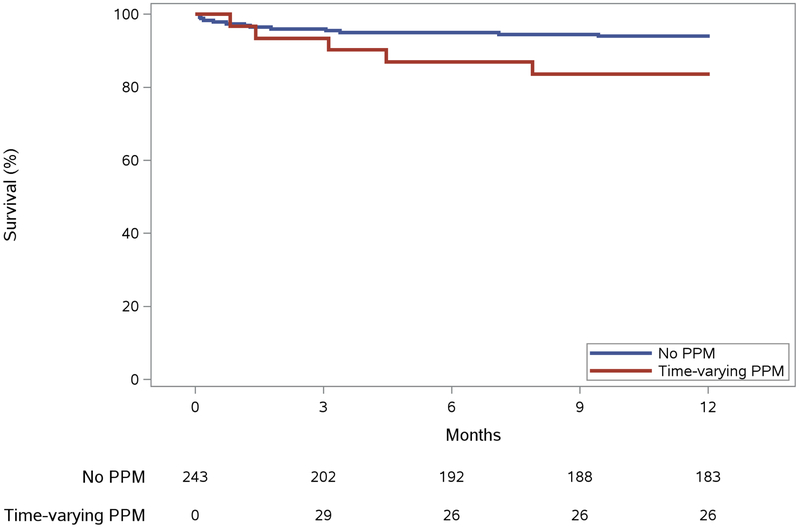
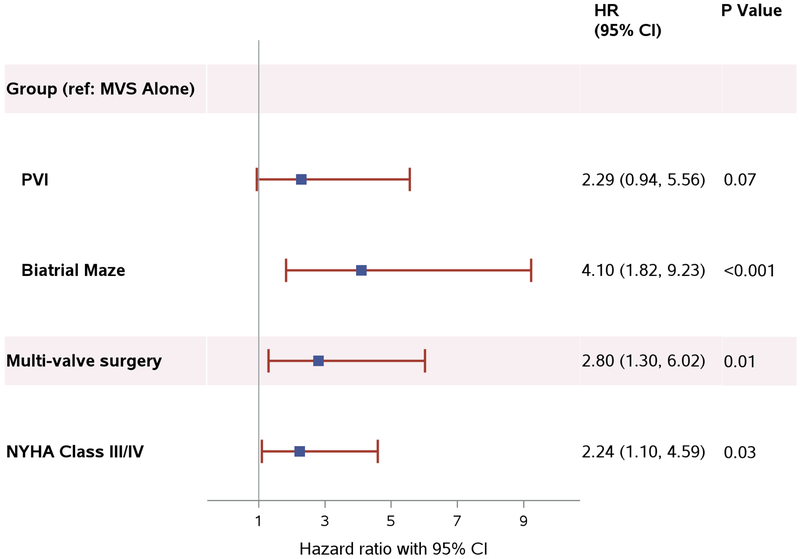
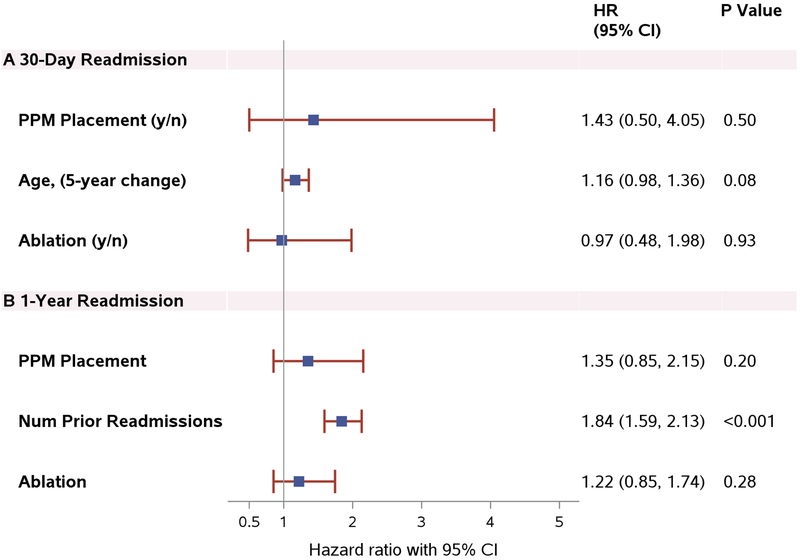
Results: Thirty-five patients received a PPM within the first year (14.4%), 29 (83%) underwent implantation during the index hospitalization. The frequency of PPM implantation was 7.7% in patients randomized to MVS alone, 16.1% in MVS + PVI, and 25% in MVS + biatrial maze. The indications for PPM were similar among patients who underwent MVS with and without ablation. Ablation, multivalve surgery, and New York Heart Association functional (NYHA) functional class III/IV were independent risk factors for PPM implantation. Length of stay post-surgery was longer in patients who received PPMs, but it was not significant when adjusted for randomization assignment (MVS vs. ablation) and age (hazard ratio [HR]: 0.81; 95% confidence interval [CI]: 0.61 to 1.08; p = 0.14). PPM implantation did not increase 30-day readmission rate (HR: 1.43; 95% CI: 0.50 to 4.05; p = 0.50). The need for PPM was associated with a higher risk of 1-year mortality (HR: 3.21; 95% CI: 1.01 to 10.17; p = 0.05) after adjustment for randomization assignment, age, and NYHA functional class.
Conclusions: AF ablation, multivalve surgery, and NYHA functional class III/IV were associated with an increased risk for permanent pacing. PPM implantation following MVS was associated with a significant increase in 1-year mortality. (Surgical Ablation Versus No Surgical Ablation for Patients With Atrial Fibrillation Undergoing Mitral Valve Surgery; NCT00903370).
Keywords: biatrial maze; cardiac surgery; permanent pacemaker; pulmonary vein isolation; valvular heart disease.
Copyright © 2019 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Pacemaker Mortality After Surgical Ablation for Atrial Fibrillation: What Is Success and Failure?J Am Coll Cardiol. 2019 May 21;73(19):2436-2438. doi: 10.1016/j.jacc.2019.03.469. J Am Coll Cardiol. 2019. PMID: 31097164 No abstract available.
References
-
- Kannel WB, Abbott RD, Savage DD, McNamara PM. Epidemiologic features of chronic atrial fibrillation: the Framingham study. N Engl J Med. 1982;306:1018–22. - PubMed
-
- Gillinov AM, Saltman AE. Ablation of atrial fibrillation with concomitant cardiac surgery. Semin Thorac Cardiovasc Surg. 2007;19:25–32. - PubMed
-
- Lee R, McCarthy PM, Wang EC, et al. Midterm survival in patients treated for atrial fibrillation: a propensity-matched comparison to patients without a history of atrial fibrillation. J Thorac Cardiovasc Surg. 2012;143:1341–51. - PubMed
-
- Gammie JS, Haddad M, Milford-Beland S, et al. Atrial fibrillation correction surgery: lessons from the Society of Thoracic Surgeons National Cardiac Database. Ann Thorac Surg. 2008;85:909–14. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
