

Home-Based Cardiac Rehabilitation: A Scientific Statement From the American Association of Cardiovascular and Pulmonary Rehabilitation, the American Heart Association, and the American College of Cardiology
- PMID: 31097258
- PMCID: PMC7341112
- DOI: 10.1016/j.jacc.2019.03.008
Home-Based Cardiac Rehabilitation: A Scientific Statement From the American Association of Cardiovascular and Pulmonary Rehabilitation, the American Heart Association, and the American College of Cardiology
Abstract
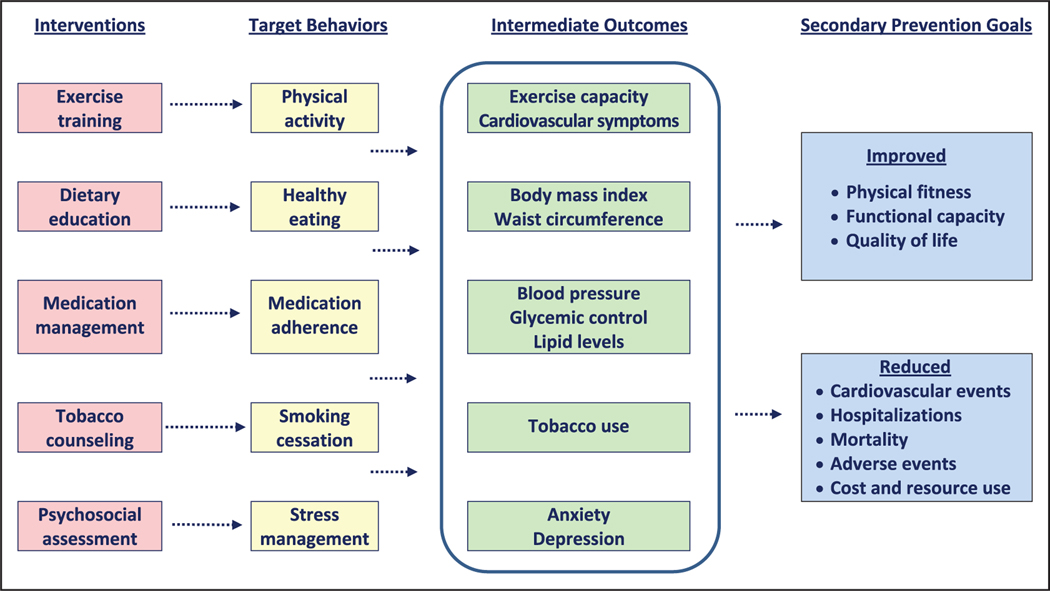
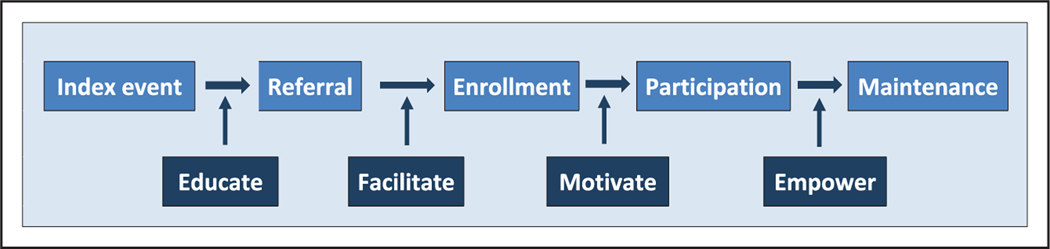
Cardiac rehabilitation (CR) is an evidence-based intervention that uses patient education, health behavior modification, and exercise training to improve secondary prevention outcomes in patients with cardiovascular disease. CR programs reduce morbidity and mortality rates in adults with ischemic heart disease, heart failure, or cardiac surgery but are significantly underused, with only a minority of eligible patients participating in CR in the United States. New delivery strategies are urgently needed to improve participation. One potential strategy is home-based CR (HBCR). In contrast to center-based CR services, which are provided in a medically supervised facility, HBCR relies on remote coaching with indirect exercise supervision and is provided mostly or entirely outside of the traditional center-based setting. Although HBCR has been successfully deployed in the United Kingdom, Canada, and other countries, most US healthcare organizations have little to no experience with such programs. The purpose of this scientific statement is to identify the core components, efficacy, strengths, limitations, evidence gaps, and research necessary to guide the future delivery of HBCR in the United States. Previous randomized trials have generated low- to moderate-strength evidence that HBCR and center-based CR can achieve similar improvements in 3- to 12-month clinical outcomes. Although HBCR appears to hold promise in expanding the use of CR to eligible patients, additional research and demonstration projects are needed to clarify, strengthen, and extend the HBCR evidence base for key subgroups, including older adults, women, underrepresented minority groups, and other higher-risk and understudied groups. In the interim, we conclude that HBCR may be a reasonable option for selected clinically stable low- to moderate-risk patients who are eligible for CR but cannot attend a traditional center-based CR program.
Keywords: AHA Scientific Statements; behavior therapy; cardiac rehabilitation; exercise; patient education.
Copyright © 2019 American Association of Cardiovascular and Pulmonary Rehabilitation, the American Heart Association, Inc., and the American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Drozda J Jr, Messer JV, Spertus J, Abramowitz B, Alexander K, Beam CT, Bonow RO, Burkiewicz JS, Crouch M, Goff DC Jr, Hellman R, James T 3rd, King ML, Machado EA Jr, Ortiz E, O’Toole M, Persell SD, Pines JM, Rybicki FJ, Sadwin LB, Sikkema JD, Smith PK, Torcson PJ, Wong JB. ACCF/ AHA/AMA-PCPI 2011 performance measures for adults with coronary artery disease and hypertension: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Performance Measures and the American Medical Association–Physician Consortium for Performance Improvement [published correction appears in Circulation. 2011;124:e39]. Circulation. 2011;124:248–270. doi: 10.1161/CIR.0b013e31821d9ef2 - DOI - PubMed
-
- Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE Jr, Chavey WE 2nd, Fesmire FM, Hochman JS, Levin TN, Lincoff AM, Peterson ED, Theroux P, Wenger NK, Wright RS. 2012 ACCF/AHA focused update incorporated into the ACCF/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines [published correction appears in Circulation. 2013;127:e863–e864]. Circulation. 2013;127:e663–e828. doi: 10.1161/CIR.0b013e31828478ac - DOI - PubMed
-
- O’Gara PT, Kushner FG, Ascheim DD, Casey DE Jr, Chung MK, de Lemos JA, Ettinger SM, Fang JC, Fesmire FM, Franklin BA, Granger CB, Krumholz HM, Linderbaum JA, Morrow DA, Newby LK, Ornato JP, Ou N, Radford MJ, Tamis-Holland JE, Tommaso CL, Tracy CM, Woo YJ, Zhao DX. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines [published correction appears in Circulation. 2013;128:e481]. Circulation. 2013;127:e362–e425. doi: 10.1161/CIR.0b013e3182742cf6 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
