

Grading Aortic Valve Stenosis With Dimensionless Index During Pre-cardiopulmonary Bypass Transesophageal Echocardiography: A Comparison With Transthoracic Echocardiography
- PMID: 31097337
- PMCID: PMC7179735
- DOI: 10.1053/j.jvca.2019.03.046
Grading Aortic Valve Stenosis With Dimensionless Index During Pre-cardiopulmonary Bypass Transesophageal Echocardiography: A Comparison With Transthoracic Echocardiography
Abstract
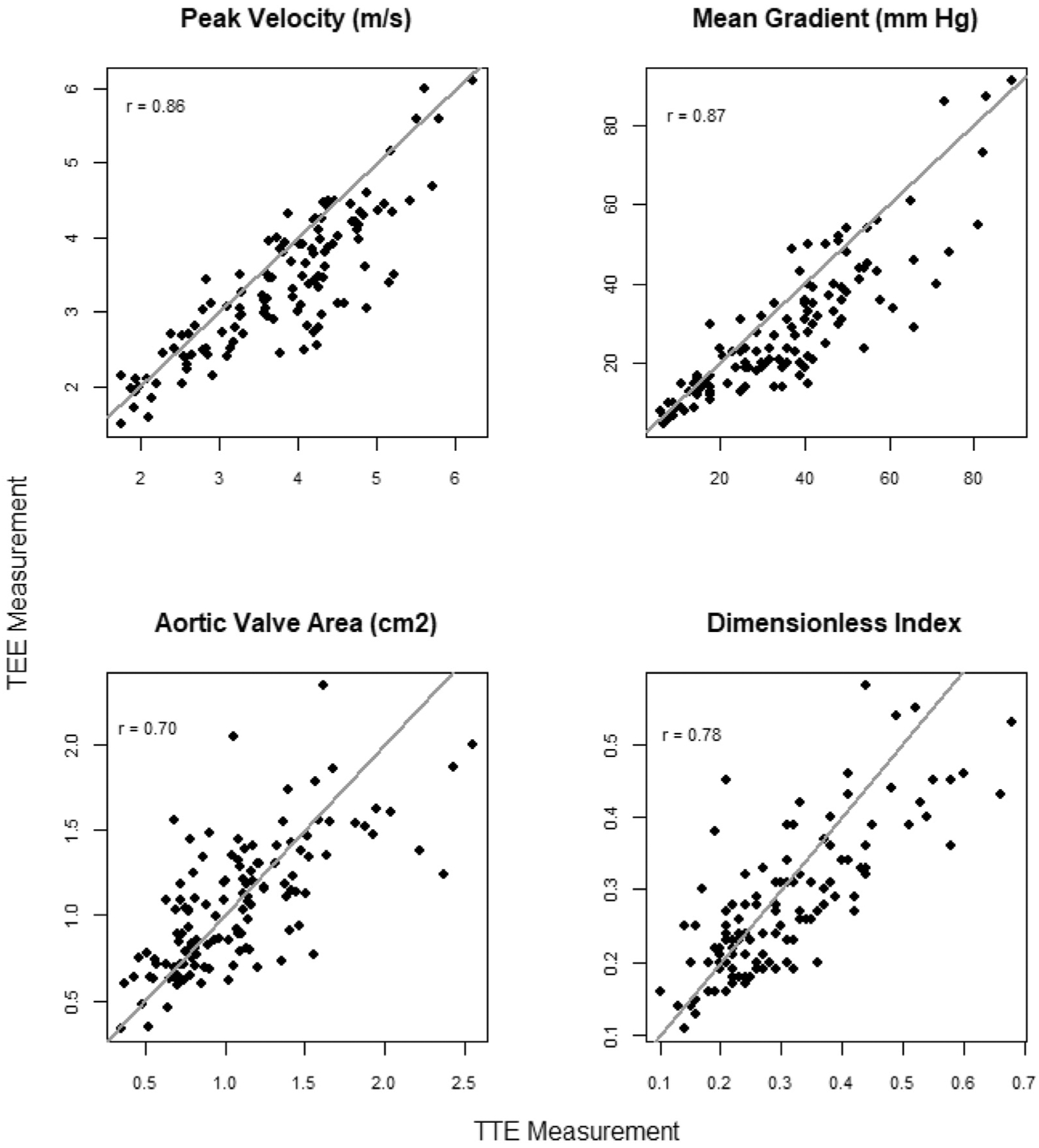
Objective: The authors hypothesized that grading valvular aortic stenosis (AS) with dimensionless index (DI) during intraoperative pre-cardiopulmonary bypass (pre-CPB) transesophageal echocardiography (TEE) would match the grade of AS during preoperative transthoracic echocardiography (TTE) for the same patients more often than when using peak velocity (Vp), mean pressure gradient (PGm), or aortic valve area (AVA).
Design: Retrospective, observational.
Setting: Single university hospital.
Participants: The participants in this study included 123 cardiac surgical patients with any degree of AS, who underwent open cardiac surgery between 2010 and 2016 at the Medical University of South Carolina and had Vp, PGm, AVA, and DI values available from reporting databases or archived imaging.
Interventions: None.
Measurements and main results: When using DI, pre-CPB TEE grading of AS severity was 1 grade higher 21.1% of the time and 1 grade lower 13.0% of the time compared with TTE, for an overall disagreement rate of 34.1%. The overall disagreement rates between pre-CPB TEE and TTE for Vp, PGm, and AVA were 39.8%, 33.3%, and 33.3%, respectively.
Conclusions: The authors could not demonstrate that DI was better than Vp, PGm, or AVA at matching AS grades between intraoperative pre-CPB TEE and preoperative TTE. When DI was used, pre-CPB TEE was more likely to overestimate than underestimate the severity of AS compared with TTE. However, when Vp or PGm was used, pre-CPB TEE was more likely to underestimate the severity of AS compared with TTE. A comprehensive approach without overemphasis on 1 parameter should be used for AS assessment by intraoperative TEE.
Keywords: aortic stenosis; dimensionless index; grading; intraoperative transesophageal echocardiography; pre-cardiopulmonary bypass transesophageal echocardiography.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of Interests
The authors have no conflicts of interest to disclose.
Figures



Comment in
-
In Pursuit of a Unicorn: Does the Ideal Parameter for Grading of Aortic Stenosis During Intraoperative Transesophageal Echocardiography Exist?J Cardiothorac Vasc Anesth. 2019 Sep;33(9):2385-2386. doi: 10.1053/j.jvca.2019.04.032. Epub 2019 May 2. J Cardiothorac Vasc Anesth. 2019. PMID: 31138469 No abstract available.
References
-
- Eltzschig HK, Rosenberger P, Loffler M, et al. Impact of intraoperative transesophageal echocardiography on surgical decisions in 12,566 patients undergoing cardiac surgery. Ann Thorac Surg 2008;85:845–52. - PubMed
-
- Karagounis A, Valencia O, Chandrasekaran V, et al. Management of patients undergoing coronary artery bypass graft surgery with mild to moderate aortic stenosis. J Heart Valve Dis 2004;13:369–73. - PubMed
-
- Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;63:2438–88. - PubMed
-
- Whitener G, McKenzie J, Akushevich I, et al. Discordance in grading methods of aortic stenosis by pre-cardiopulmonary bypass transesophageal echocardiography. Anesth Analg 2016;122:953–8. - PubMed
-
- Whitener G, Sivak J, Akushevich I, et al. Grading aortic stenosis with mean gradient and aortic valve area: A comparison between preoperative transthoracic and precardiopulmonary bypass transesophageal echocardiography. J Cardiothorac Vasc Anesth 2016;30:1254–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
