

Causal Factors for Knee, Hip, and Hand Osteoarthritis: A Mendelian Randomization Study in the UK Biobank
- PMID: 31099188
- PMCID: PMC6790695
- DOI: 10.1002/art.40928
Causal Factors for Knee, Hip, and Hand Osteoarthritis: A Mendelian Randomization Study in the UK Biobank
Abstract
Objective: There is no curative treatment for osteoarthritis (OA), which is the most common form of arthritis. This study was undertaken to identify causal risk factors of knee, hip, and hand OA.
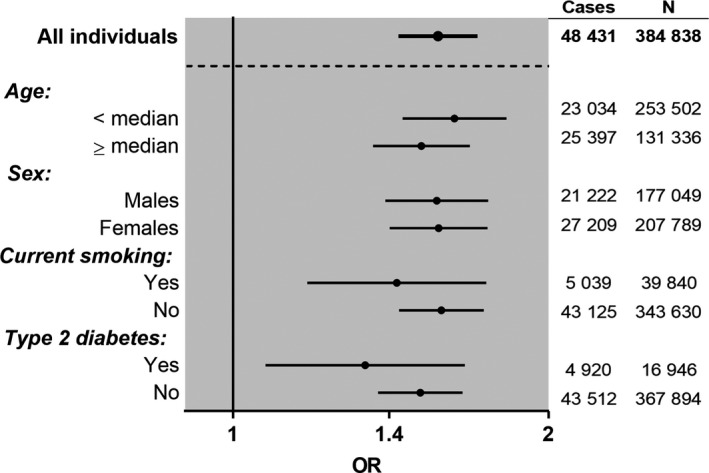
Methods: Individual-level data from 384,838 unrelated participants in the UK Biobank study were analyzed. Mendelian randomization (MR) analyses were performed to test for causality for body mass index (BMI), bone mineral density (BMD), serum high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, and triglyceride levels, type 2 diabetes, systolic blood pressure (BP), and C-reactive protein (CRP) levels. The primary outcome measure was OA determined using hospital diagnoses (all sites, n = 48,431; knee, n = 19,727; hip, n = 11,875; hand, n = 2,330). Odds ratios (ORs) with 95% confidence intervals (95% CIs) were calculated.
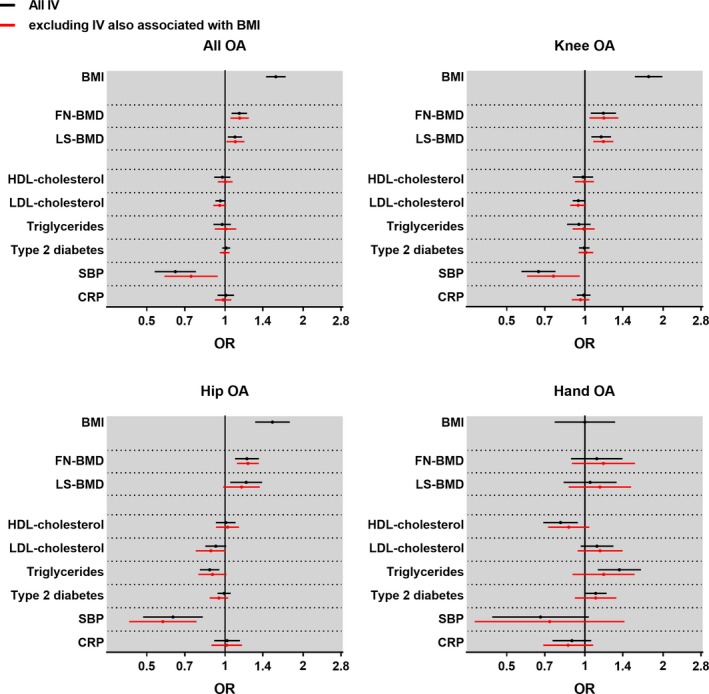
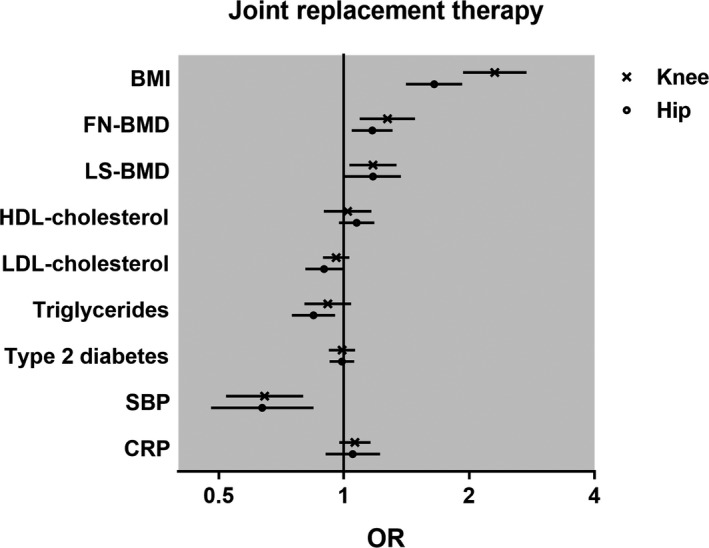
Results: MR analyses demonstrated a robust causal association of genetically determined BMI with all OA (OR per SD increase 1.57 [95% CI 1.44-1.71]), and with knee OA and hip OA, but not with hand OA. Increased genetically determined femoral neck BMD was causally associated with all OA (OR per SD increase 1.14 [95% CI 1.06-1.22]), knee OA, and hip OA. Low systolic BP was causally associated with all OA (OR per SD decrease 1.55 [95% CI 1.29-1.87]), knee OA, and hip OA. There was no evidence of causality for the other tested metabolic factors or CRP level.
Conclusion: Our findings indicate that BMI exerts a major causal effect on the risk of OA at weight-bearing joints, but not at the hand. Evidence of causality of all OA, knee OA, and hip OA was also observed for high femoral neck BMD and low systolic BP. However, we found no evidence of causality for other metabolic factors or CRP level.
© 2019 The Authors. Arthritis & Rheumatology published by Wiley Periodicals, Inc. on behalf of American College of Rheumatology.
Figures
Comment in
-
High Blood Pressure and Osteoarthritis: Friends or Foes? Comment on the Article by Funck-Brentano et al.Arthritis Rheumatol. 2019 Dec;71(12):2131-2132. doi: 10.1002/art.41086. Epub 2019 Oct 21. Arthritis Rheumatol. 2019. PMID: 31430062 No abstract available.
-
Reply.Arthritis Rheumatol. 2019 Dec;71(12):2132. doi: 10.1002/art.41087. Epub 2019 Oct 16. Arthritis Rheumatol. 2019. PMID: 31436027 No abstract available.
References
-
- Arden N, Nevitt MC. Osteoarthritis: epidemiology. Best Pract Res Clin Rheumatol 2006;20:3–25. - PubMed
-
- Cooper C, Snow S, McAlindon TE, Kellingray S, Stuart B, Coggon D, et al. Risk factors for the incidence and progression of radiographic knee osteoarthritis. Arthritis Rheum 2000;43:995–1000. - PubMed
-
- Bijlsma JW, Berenbaum F, Lafeber FP. Osteoarthritis: an update with relevance for clinical practice. Lancet 2011;377:2115–26. - PubMed
-
- Lohmander LS, Gerhardsson de Verdier M, Rollof J, Nilsson PM, Engström G. Incidence of severe knee and hip osteoarthritis in relation to different measures of body mass: a population‐based prospective cohort study. Ann Rheum Dis 2009;68:490–6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
