

The benefits of extrinsic ligament release for potentially hemodynamically unstable pancreaticoduodenal arcade aneurysm with median arcuate ligament syndrome: a case report
- PMID: 31101073
- PMCID: PMC6525411
- DOI: 10.1186/s12893-019-0514-8
The benefits of extrinsic ligament release for potentially hemodynamically unstable pancreaticoduodenal arcade aneurysm with median arcuate ligament syndrome: a case report
Abstract
Background: A pancreaticoduodenal artery aneurysm (PDAA) occurring in close association with median arcuate ligament syndrome (MALS) is rare. A surgical procedure, such as median arcuate ligament (MAL) release, should be considered in such cases, but the operative criteria remain unknown. In this study, we reported an extremely rare case of PDAA with periarteritis nodosa (PAN) and MALS.
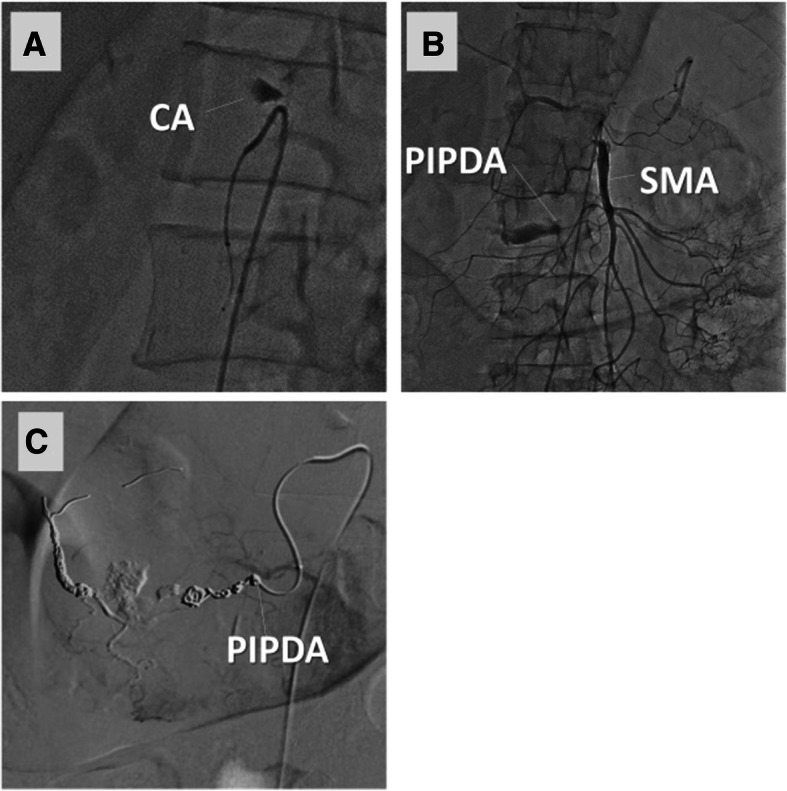
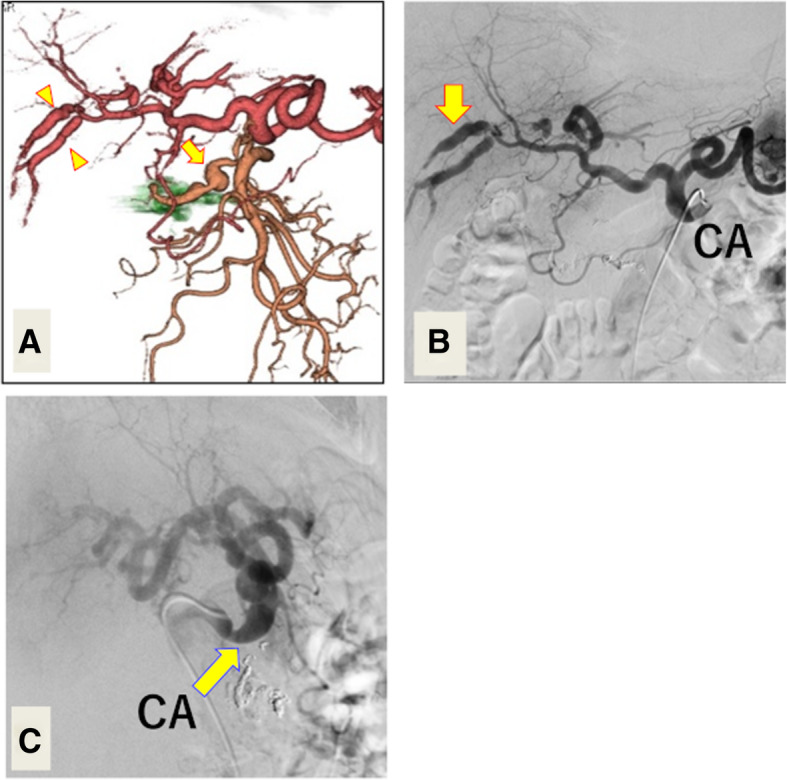
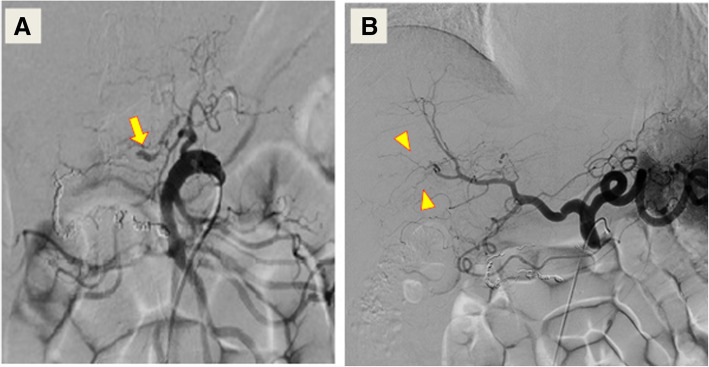
Case presentation: A 60-year-old man was transferred to our department with sudden onset of abdominal pain. We initially diagnosed his condition as a PDAA rupture with MALS based on enhanced computed tomography (CT). We promptly performed transcatheter arterial embolization (TAE) of PDAA, and the angiogram showed stagnant contrast agent in the celiac trunk, indicating total celiac artery occlusion. Follow-up enhanced CT three weeks after the first TAE clearly demonstrated newly formed, multiple aneurysms in the pancreaticoduodenal arcade and the hepatic artery. These findings indicated a systemic disorder, such as PAN or segmental arterial mediolysis, as the underlying cause. Therefore, we started corticosteroid therapy and performed diagnostic angiography to clarify the celiac artery's patency. Contrary to the initial angiography, the second angiography showed sustained blood flow in the celiac artery. Nevertheless, we performed both extrinsic MAL release and consecutive TAE because of the risk of multiple aneurysms rupturing due to an uncontrolled systemic disorder and consequent hepatic ischemia. The patient had no episode of recurrence until one year of follow-up.
Conclusions: It is important to evaluate risk for hemodynamically unstable events to decide the best treatment strategy for MALS.
Keywords: Case report; Extrinsic median arcuate ligament release; Median arcuate ligament syndrome; Pancreaticoduodenal arcade; Pancreaticoduodenal artery aneurysm.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Mano Y, Takehara Y, Sakaguchi T, Alley MT, Isoda H, Shimizu T, et al. Hemodynamic assessment of celiaco-mesenteric anastomosis in patients with pancreaticoduodenal artery aneurysm concomitant with celiac artery occlusion using flow-sensitive four-dimensional magnetic resonance imaging. Eur J Vasc Endovasc Surg. 2013;46:321–328. doi: 10.1016/j.ejvs.2013.06.011. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
