

Preoperative chronic beta-blocker prescription in elderly patients as a risk factor for postoperative mortality stratified by preoperative blood pressure: a cohort study
- PMID: 31101323
- PMCID: PMC6676243
- DOI: 10.1016/j.bja.2019.03.042
Preoperative chronic beta-blocker prescription in elderly patients as a risk factor for postoperative mortality stratified by preoperative blood pressure: a cohort study
Abstract
Background: Recent data suggest that beta blockers are associated with increased perioperative risk in hypertensive patients. We investigated whether beta blockers were associated with an increased risk in elderly patients with raised preoperative arterial blood pressure.
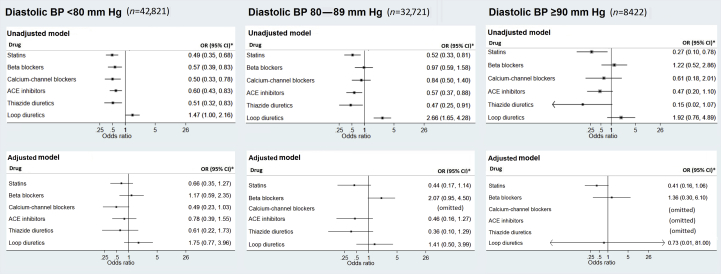
Methods: We conducted a propensity-score-matched cohort study of primary care data from the UK Clinical Practice Research Datalink (2004-13), including 84 633 patients aged 65 yr or over. Conditional logistic regression models, including factors that were significantly associated with the outcome, were constructed for 30-day mortality after elective noncardiac surgery. The effects of beta blockers (primary outcome), renin-angiotensin system (RAS) inhibitors, calcium-channel blockers, thiazides, loop diuretics, and statins were investigated at systolic and diastolic arterial pressure thresholds.
Results: Beta blockers were associated with increased odds of postoperative 30-day mortality in patients with systolic hypertension (defined as systolic BP >140 mm Hg; adjusted odds ratio [aOR]: 1.92; 95% confidence interval [CI]: 1.05-3.51). After excluding patients for whom prior data suggest benefit from perioperative beta blockade (patients with prior myocardial infarction or heart failure), rather than adjusting for them, the point estimate shifted slightly (aOR: 2.06; 95% CI: 1.09-3.89). Compared with no use, statins (aOR: 0.35; 95% CI: 0.17-0.75) and thiazides (aOR: 0.28; 95% CI: 0.10-0.78) were associated with lower mortality in patients with systolic hypertension.
Conclusions: These data suggest that the safety of perioperative beta blockers may be influenced by preoperative blood pressure thresholds. A randomised controlled trial of beta-blocker withdrawal, in select populations, is required to identify a causal relationship.
Keywords: beta blocker; blood pressure; hypertension; mortality; perioperative outcome; risk factors; surgery.
Copyright © 2019 British Journal of Anaesthesia. Published by Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures


Comment in
-
Perioperative beta-adrenergic antagonism: panacea or poison?Br J Anaesth. 2019 Aug;123(2):97-100. doi: 10.1016/j.bja.2019.05.039. Epub 2019 Jun 24. Br J Anaesth. 2019. PMID: 31248641 Free PMC article. No abstract available.
References
-
- Blessberger H., Kammler J., Domanovits H. Perioperative beta-blockers for preventing surgery-related mortality and morbidity. Cochrane Database Syst Rev. 2014;9:CD004476. - PubMed
-
- Jorgensen M.E., Andersson C., Venkatesan S., Sanders R.D. Beta-blockers in noncardiac surgery: did observational studies put us back on safe ground? Br J Anaesth. 2018;121:16–25. - PubMed
-
- Devereaux P.J., Yang H., Yusuf S. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): a randomised controlled trial. Lancet. 2008;371:1839–1847. - PubMed
-
- Jorgensen M.E., Sanders R.D., Kober L. Beta-blocker subtype and risks of perioperative adverse events following non-cardiac surgery: a nationwide cohort study. Eur Heart J. 2017;38:2421–2428. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
