

Estimating Lifetime Benefits Associated with Immuno-Oncology Therapies: Challenges and Approaches for Overall Survival Extrapolations
- PMID: 31102143
- PMCID: PMC6830404
- DOI: 10.1007/s40273-019-00806-4
Estimating Lifetime Benefits Associated with Immuno-Oncology Therapies: Challenges and Approaches for Overall Survival Extrapolations
Abstract
Background: Standard parametric survival models are commonly used to estimate long-term survival in oncology health technology assessments; however, they can inadequately represent the complex pattern of hazard functions or underlying mechanism of action (MoA) of immuno-oncology (IO) treatments.
Objective: The aim of this study was to explore methods for extrapolating overall survival (OS) and provide insights on model selection in the context of the underlying MoA of IO treatments.
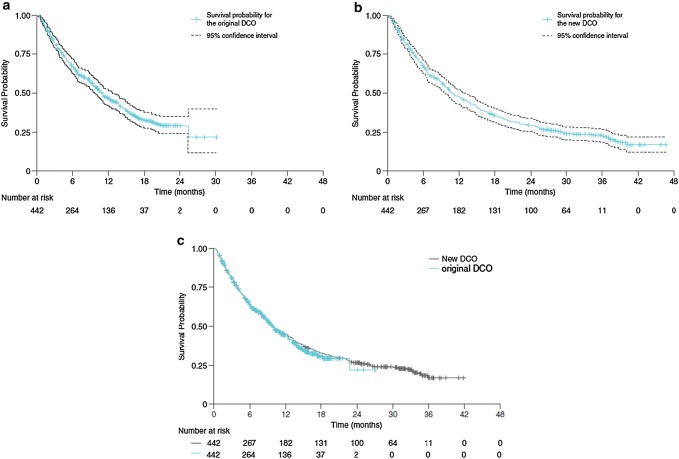
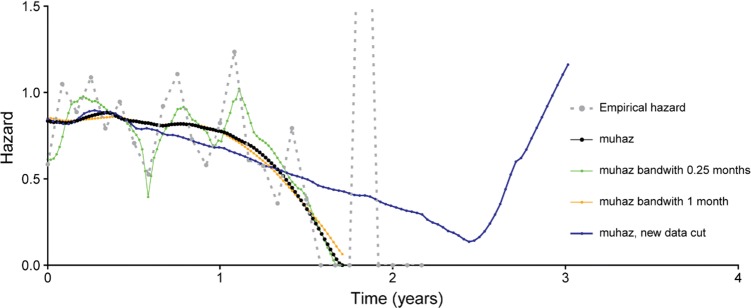
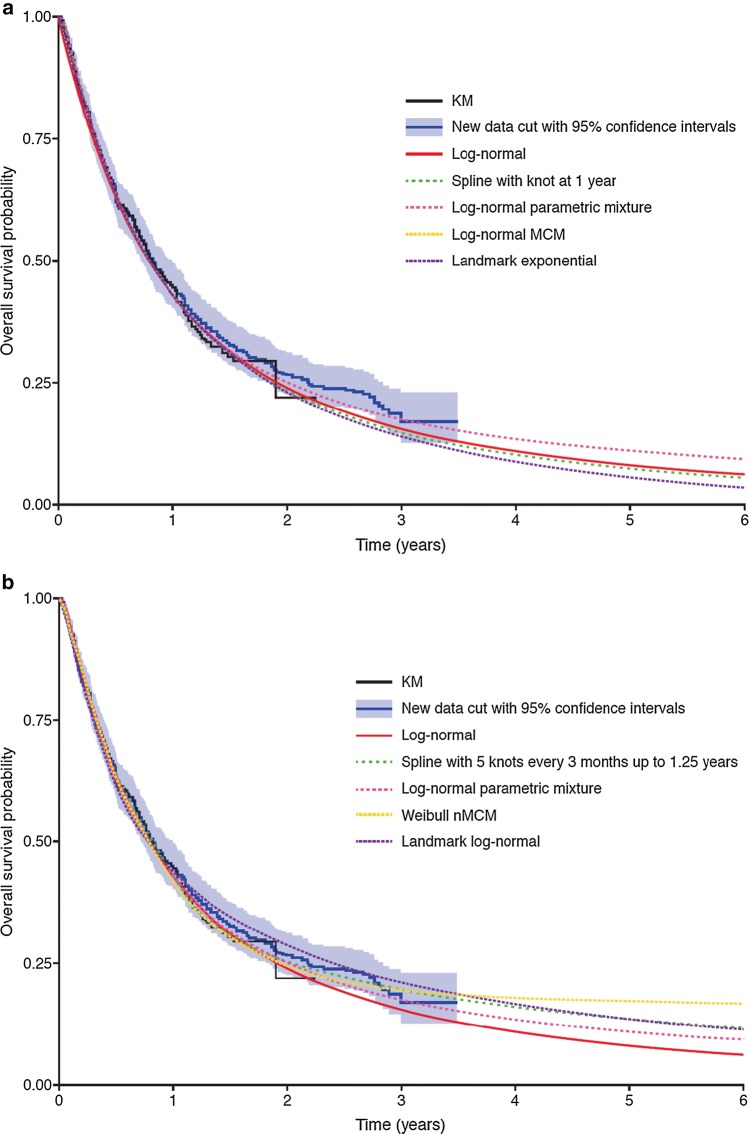
Methods: Standard parametric, flexible parametric, cure, parametric mixture and landmark models were applied to data from ATLANTIC (NCT02087423; data cut-off [DCO] 3 June 2016). The goodness of fit of each model was compared using the observed survival and hazard functions, together with the plausibility of corresponding model extrapolation beyond the trial period. Extrapolations were compared with updated data from ATLANTIC (DCO 7 November 2017) for validation.
Results: A close fit to the observed OS was seen with all models; however, projections beyond the trial period differed. Estimated mean OS differed substantially across models. The cure models provided the best fit for the new DCO.
Conclusions: Standard parametric models fitted to the initial ATLANTIC DCO generally underestimated longer-term OS, compared with the later DCO. Cure, parametric mixture and response-based landmark models predicted that larger proportions of patients with metastatic non-small cell lung cancer receiving IO treatments may experience long-term survival, which was more in keeping with the observed data. Further research using more mature OS data for IO treatments is needed.
Conflict of interest statement
Mario J.N.M. Ouwens and Pralay Mukhopadhyay are employees of AstraZeneca. Yiduo Zhang is an employee of AstraZeneca and owns stock in AstraZeneca. Min Huang is a former employee of AstraZeneca. Nicholas Latimer has received consultancy fees from AstraZeneca in relation to material presented in this manuscript, and has also received consultancy fees from Bristol-Myers Squibb and Pfizer for providing modelling advice. Andrew Briggs has received consultancy fees from AstraZeneca in relation to material presented in this manuscript, and has also received consultancy fees from Bristol-Myers Squibb and Merck (who are manufacturers of immuno-oncologic therapies).
Figures
References
-
- National Institute for Health and Care Excellence (NICE). Guide to the methods of technology appraisal. London: NICE; 2013. - PubMed
-
- Briggs A, Claxton K, Sculpher M. Decision modelling for health economic evaluation. New York: Oxford University Press Inc.; 2006.
-
- Sanders GD, Neumann PJ, Basu A, Brock DW, Feeny D, Krahn M, et al. Recommendations for conduct, methodological practices, and reporting of cost-effectiveness analyses: second panel on cost-effectiveness in health and medicine. JAMA. 2016;316(10):1093‒103. - PubMed
-
- Canadian Agency for Drugs and Technologies in Health . Guidelines for the economic evaluation of health technologies: Canada. 4. Ottawa: Canadian Agency for Drugs and Technologies in Health; 2017.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
